Department of Research, Audit, Innovation, & Development (RAID), East Anglian Air Ambulance, Norwich, UK
Emergency Department, Addenbrooke's Hospital, Cambridge, UK.
Emerg Med J. 2020 Nov;37(11):674-679. doi: 10.1136/emermed-2019-209077. Epub 2020 Sep 14.
In the UK, 20% of patients with severe traumatic brain injury (TBI) receive prehospital emergency anaesthesia (PHEA). Current guidance recommends an end-tidal carbon dioxide (ETCO) of 4.0-4.5 kPa (30.0-33.8 mm Hg) to achieve a low-normal arterial partial pressure of CO (PaCO), and reduce secondary brain injury. This recommendation assumes a 0.5 kPa (3.8 mm Hg) ETCO-PaCO gradient. However, the gradient in the acute phase of TBI is unknown. The primary aim was to report the ETCO-PaCO gradient of TBI patients at hospital arrival.
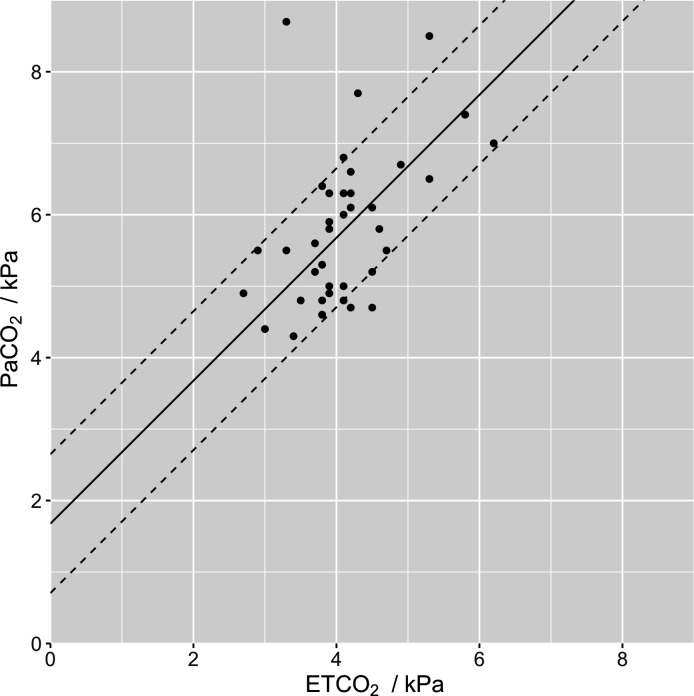
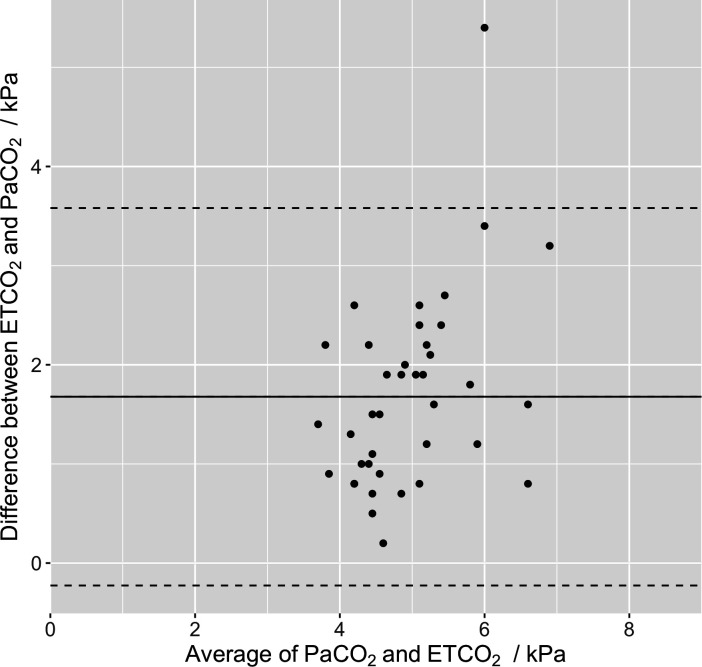
A retrospective cohort study of adult patients with serious TBI, who received a PHEA by a prehospital critical care team in the East of England between 1 April 2015 and 31 December 2017. Linear regression was performed to test for correlation and reported as R-squared (R). A Bland-Altman plot was used to test for paired ETCO and PaCO agreement and reported with 95% CI. ETCO-PaCO gradient data were compared with a two-tailed, unpaired, t-test.
107 patients were eligible for inclusion. Sixty-seven patients did not receive a PaCO sample within 30 min of hospital arrival and were therefore excluded. Forty patients had complete data and were included in the final analysis; per protocol. The mean ETCO-PaCO gradient was 1.7 (±1.0) kPa (12.8 mm Hg), with moderate correlation (R=0.23, p=0.002). The Bland-Altman bias was 1.7 (95% CI 1.4 to 2.0) kPa with upper and lower limits of agreement of 3.6 (95% CI 3.0 to 4.1) kPa and -0.2 (95% CI -0.8 to 0.3) kPa, respectively. There was no evidence of a larger gradient in more severe TBI (p=0.29). There was no significant gradient correlation in patients with a coexisting serious thoracic injury (R=0.13, p=0.10), and this cohort had a larger ETCO-PaCO gradient, 2.0 (±1.1) kPa (15.1 mm Hg), p=0.01. Patients who underwent prehospital arterial blood sampling had an arrival PaCO of 4.7 (±0.2) kPa (35.1 mm Hg).
There is only moderate correlation of ETCO and PaCO at hospital arrival in patients with serious TBI. The mean ETCO-PaCO gradient was 1.7 (±1.0) kPa (12.8 mm Hg). Lower ETCO targets than previously recommended may be safe and appropriate, and there may be a role for prehospital PaCO measurement.
在英国,20%的严重创伤性脑损伤(TBI)患者接受院前急救麻醉(PHEA)。目前的指南建议呼气末二氧化碳(ETCO)为 4.0-4.5kPa(30.0-33.8mmHg)以达到低正常动脉二氧化碳分压(PaCO),从而减少继发性脑损伤。这一建议假设 ETCO-PaCO 梯度为 0.5kPa(3.8mmHg)。然而,TBI 急性期的梯度尚不清楚。主要目的是报告 TBI 患者入院时的 ETCO-PaCO 梯度。
这是一项回顾性队列研究,纳入了 2015 年 4 月 1 日至 2017 年 12 月 31 日期间在英格兰东部接受院前急救重症监护团队治疗的严重 TBI 成年患者。采用线性回归检验 ETCO 和 PaCO 的相关性,并以 R 平方(R)表示。采用 Bland-Altman 图检验 ETCO 和 PaCO 的配对一致性,并以 95%CI 表示。ETCO-PaCO 梯度数据与双侧、非配对 t 检验进行比较。
共有 107 例患者符合纳入标准。67 例患者在入院后 30 分钟内未采集 PaCO 样本,因此被排除。40 例患者有完整的数据,符合纳入标准。平均 ETCO-PaCO 梯度为 1.7(±1.0)kPa(12.8mmHg),相关性适中(R=0.23,p=0.002)。Bland-Altman 偏倚为 1.7(95%CI 1.4-2.0)kPa,上下限分别为 3.6(95%CI 3.0-4.1)kPa 和 -0.2(95%CI -0.8-0.3)kPa。严重 TBI 患者的梯度无明显增大(p=0.29)。合并严重胸部损伤的患者无明显的 ETCO-PaCO 梯度相关性(R=0.13,p=0.10),且该队列的 ETCO-PaCO 梯度更大,为 2.0(±1.1)kPa(15.1mmHg),p=0.01。行院前动脉采血的患者入院时 PaCO 为 4.7(±0.2)kPa(35.1mmHg)。
严重 TBI 患者入院时 ETCO 和 PaCO 的相关性仅为中度。平均 ETCO-PaCO 梯度为 1.7(±1.0)kPa(12.8mmHg)。低于先前推荐的 ETCO 目标可能是安全和合适的,并且院前 PaCO 测量可能有一定作用。