Yigezu Amanuel, Alemayehu Senait, Hamusse Shallo Daba, Ergeta Getachew Teshome, Hailemariam Damen, Hailu Alemayehu
School of Public Health, Addis Ababa University, Addis Ababa, Ethiopia.
Ethiopian Public Health Institute, Addis Ababa, Ethiopia.
Cost Eff Resour Alloc. 2020 Sep 11;18:34. doi: 10.1186/s12962-020-00231-x. eCollection 2020.
Globally, there is a consensus to end the HIV/AIDS epidemic by 2030, and one of the strategies to achieve this target is that 90% of people living with HIV should know their HIV status. Even if there is strong evidence of clients' preference for testing in the community, HIV voluntary counseling and testing (VCT) continue to be undertaken predominantly in health facilities. Hence, empirical cost-effectiveness evidence about different HIV counseling and testing models is essential to inform whether such community-based testing are justifiable compared with additional resources required. Therefore, the purpose of this study was to compare the cost-effectiveness of facility-based, stand-alone and mobile-based HIV voluntary counseling and testing methods in Addis Ababa, Ethiopia.
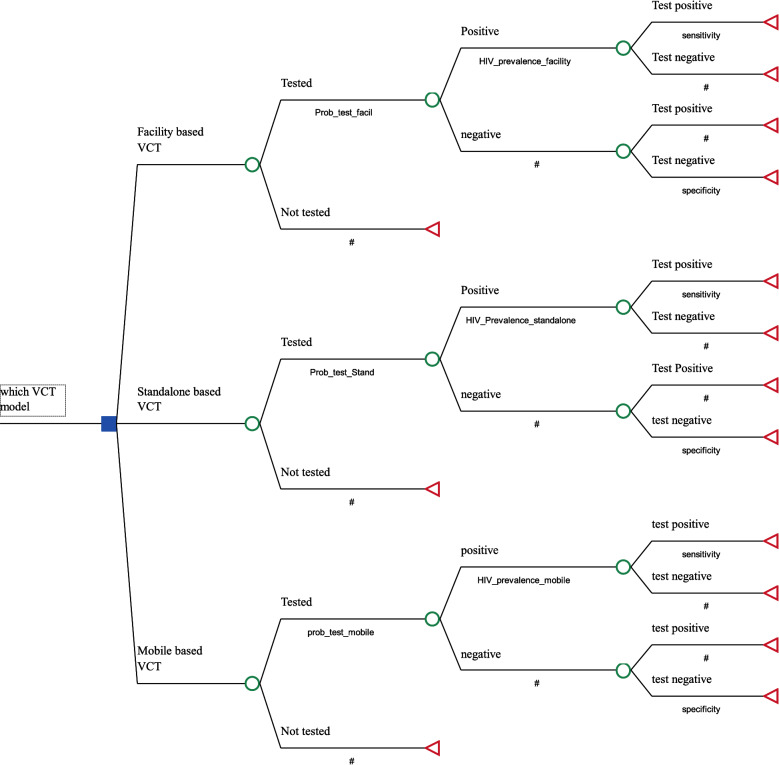
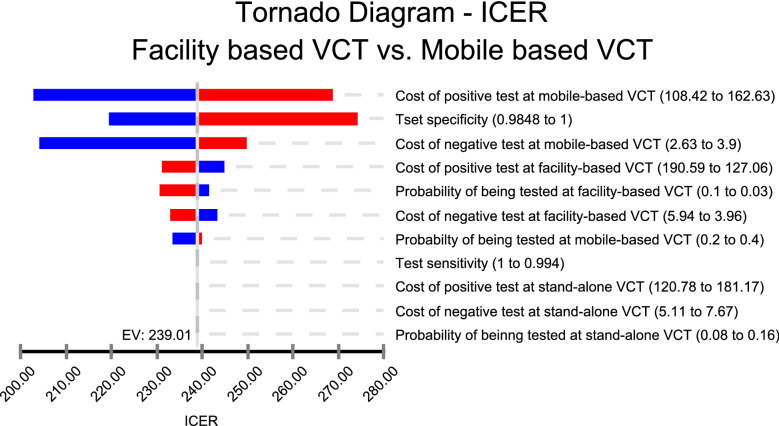
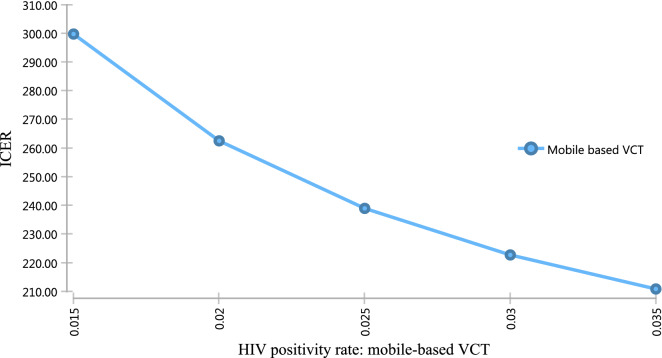
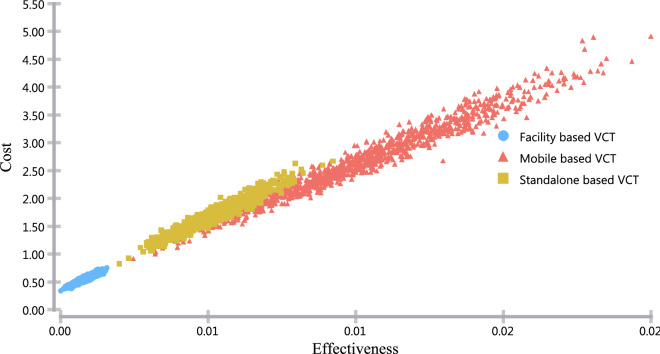
Annual economic costs of counseling and testing methods were collected from the providers' perspective from July 2016 to June 2017. Ingredients based bottom-up costing approach was applied. The effectiveness of the interventions was measured in terms of the number of HIV seropositive clients identified. Decision tree modeling was built using TreeAge Pro 2018 software, and one-way and probabilistic sensitivity analyses were conducted by varying HIV positivity rate, costs, and probabilities.
The cost of test per client for facility-based, stand-alone and mobile-based VCT was $5.06, $6.55 and $3.35, respectively. The unit costs of test per HIV seropositive client for the corresponding models were $158.82, $150.97 and $135.82, respectively. Of the three models, stand-alone-based VCT was extendedly dominated. Mobile-based VCT costs, an additional cost of USD 239 for every HIV positive client identified when compared to facility-based VCT.
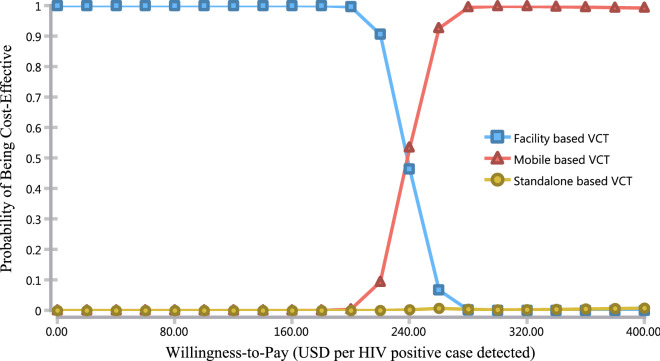
Using a mobile-based VCT approach costs less than both the facility-based and stand-alone approaches, in terms of both unit cost per tested individual and unit cost per HIV seropositive cases identified. The stand-alone VCT approach was not cost-effective compared to facility-based and mobile-based VCT. The incremental cost-effectiveness ratio for mobile-based VCT compared with facility-based VCT was USD 239 per HIV positive case.
在全球范围内,人们已达成到2030年终结艾滋病毒/艾滋病流行的共识,实现这一目标的策略之一是90%的艾滋病毒感染者应知晓自己的感染状况。即便有确凿证据表明服务对象倾向于在社区进行检测,但艾滋病毒自愿咨询检测(VCT)仍主要在医疗机构开展。因此,关于不同艾滋病毒咨询检测模式的实证成本效益证据对于判断与所需额外资源相比,此类基于社区的检测是否合理至关重要。所以,本研究的目的是比较埃塞俄比亚亚的斯亚贝巴基于医疗机构、独立式和移动式的艾滋病毒自愿咨询检测方法的成本效益。
从提供者角度收集2016年7月至2017年6月咨询检测方法的年度经济成本。采用基于成分的自下而上成本核算方法。干预措施的有效性通过检测出的艾滋病毒血清阳性服务对象数量来衡量。使用TreeAge Pro 2018软件构建决策树模型,并通过改变艾滋病毒阳性率、成本和概率进行单向和概率敏感性分析。
基于医疗机构、独立式和移动式VCT的每位服务对象检测成本分别为5.06美元、6.55美元和3.35美元。相应模式下每位艾滋病毒血清阳性服务对象的检测单位成本分别为158.82美元、150.97美元和135.82美元。在这三种模式中,独立式VCT被广泛占优。与基于医疗机构的VCT相比,移动式VCT每检测出一名艾滋病毒阳性服务对象要额外花费239美元。
就每位受检个体的单位成本以及每例检测出的艾滋病毒血清阳性病例的单位成本而言,采用移动式VCT方法的成本低于基于医疗机构和独立式的方法。与基于医疗机构和移动式的VCT相比,独立式VCT方法不具有成本效益。移动式VCT与基于医疗机构的VCT相比,每例艾滋病毒阳性病例的增量成本效益比为239美元。