Neilan Anne M, Losina Elena, Bangs Audrey C, Flanagan Clare, Panella Christopher, Eskibozkurt G Ege, Mohareb Amir, Hyle Emily P, Scott Justine A, Weinstein Milton C, Siedner Mark J, Reddy Krishna P, Harling Guy, Freedberg Kenneth A, Shebl Fatma M, Kazemian Pooyan, Ciaranello Andrea L
Division of General Academic Pediatrics, Department of Pediatrics, Massachusetts General Hospital, Boston, Massachusetts, USA.
Division of Infectious Diseases, Department of Medicine, Massachusetts General Hospital, Boston, Massachusetts, USA.
Clin Infect Dis. 2021 Nov 2;73(9):e2908-e2917. doi: 10.1093/cid/ciaa1418.
We projected the clinical and economic impact of alternative testing strategies on coronavirus disease 2019 (COVID-19) incidence and mortality in Massachusetts using a microsimulation model.
We compared 4 testing strategies: (1) hospitalized: polymerase chain reaction (PCR) testing only for patients with severe/critical symptoms warranting hospitalization; (2) symptomatic: PCR for any COVID-19-consistent symptoms, with self-isolation if positive; (3) symptomatic + asymptomatic once: symptomatic and 1-time PCR for the entire population; and (4) symptomatic + asymptomatic monthly: symptomatic with monthly retesting for the entire population. We examined effective reproduction numbers (Re = 0.9-2.0) at which policy conclusions would change. We assumed homogeneous mixing among the Massachusetts population (excluding those residing in long-term care facilities). We used published data on disease progression and mortality, transmission, PCR sensitivity/specificity (70%/100%), and costs. Model-projected outcomes included infections, deaths, tests performed, hospital-days, and costs over 180 days, as well as incremental cost-effectiveness ratios (ICERs, $/quality-adjusted life-year [QALY]).
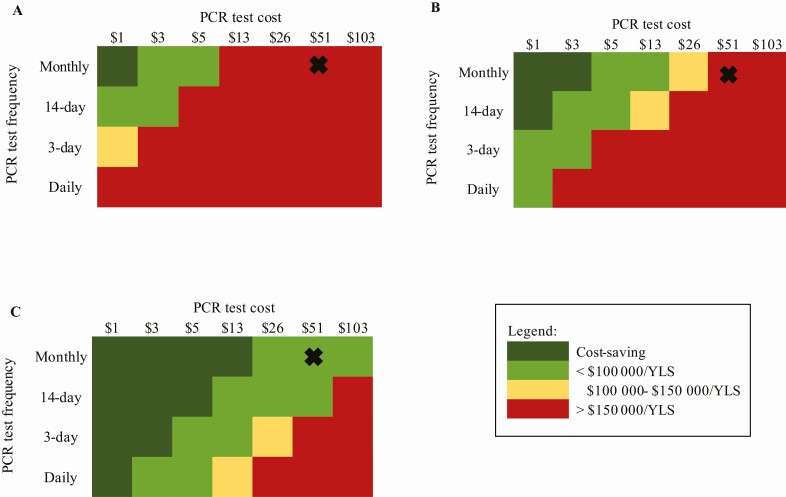
At Re = 0.9, symptomatic + asymptomatic monthly vs hospitalized resulted in a 64% reduction in infections and a 46% reduction in deaths, but required >66-fold more tests/day with 5-fold higher costs. Symptomatic + asymptomatic monthly had an ICER <$100 000/QALY only when Re ≥1.6; when test cost was ≤$3, every 14-day testing was cost-effective at all Re examined.
Testing people with any COVID-19-consistent symptoms would be cost-saving compared to testing only those whose symptoms warrant hospital care. Expanding PCR testing to asymptomatic people would decrease infections, deaths, and hospitalizations. Despite modest sensitivity, low-cost, repeat screening of the entire population could be cost-effective in all epidemic settings.
我们使用微观模拟模型预测了替代检测策略对马萨诸塞州2019冠状病毒病(COVID-19)发病率和死亡率的临床及经济影响。
我们比较了4种检测策略:(1)住院患者:仅对有严重/危急症状需住院治疗的患者进行聚合酶链反应(PCR)检测;(2)有症状者:对任何符合COVID-19症状的患者进行PCR检测,检测呈阳性则自我隔离;(3)有症状者+无症状者一次检测:对全体人群进行有症状者检测和1次PCR检测;(4)有症状者+无症状者每月检测:对全体人群进行有症状者检测并每月重新检测。我们研究了有效再生数(Re = 0.9 - 2.0),在该数值下政策结论会发生变化。我们假设马萨诸塞州人群(不包括居住在长期护理机构的人)之间混合均匀。我们使用了已发表的关于疾病进展和死亡率、传播、PCR敏感性/特异性(70%/100%)以及成本的数据。模型预测的结果包括180天内的感染数、死亡数、检测次数、住院天数和成本,以及增量成本效益比(ICERs,美元/质量调整生命年[QALY])。
在Re = 0.9时,有症状者+无症状者每月检测与仅检测住院患者相比,感染数减少了64%,死亡数减少了46%,但每天所需检测次数增加了66倍以上,成本增加了5倍。仅当Re≥1.6时,有症状者+无症状者每月检测的ICER <100,000美元/QALY;当检测成本≤3美元时,在所有研究的Re值下,每14天进行一次检测都具有成本效益。
与仅检测那些症状需要住院治疗的人相比,对任何符合COVID-19症状的人进行检测将节省成本。将PCR检测扩展到无症状人群将减少感染、死亡和住院人数。尽管敏感性一般,但对全体人群进行低成本、重复筛查在所有疫情情况下都可能具有成本效益。