Kirchweger Patrick, Wundsam Helwig Valentin, Fischer Ines, Rösch Christiane Sophie, Böhm Gernot, Tsybrovskyy Oleksiy, Alibegovic Vedat, Függer Reinhold
Department of General and Visceral Surgery, Ordensklinikum Linz - Barmherzige Schwestern, Linz, Austria.
Medical Faculty, Johannes Kepler University Linz, Linz, Austria.
World J Surg Oncol. 2020 Sep 18;18(1):248. doi: 10.1186/s12957-020-02016-1.
Ganglioneuromas (GNs) are extremely rare, slowly growing, benign tumors that can arise from Schwann cells, ganglion cells, and neuronal or fibrous tissues. Due to their origin from the sympathetic neural crest, they show neuroendocrine potential; however, most are reported to be hormonally inactive. Nevertheless, complete surgical removal is recommended for symptom control or for the prevention of potential malignant degeneration.
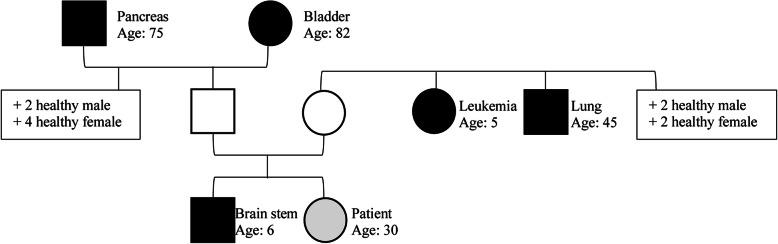
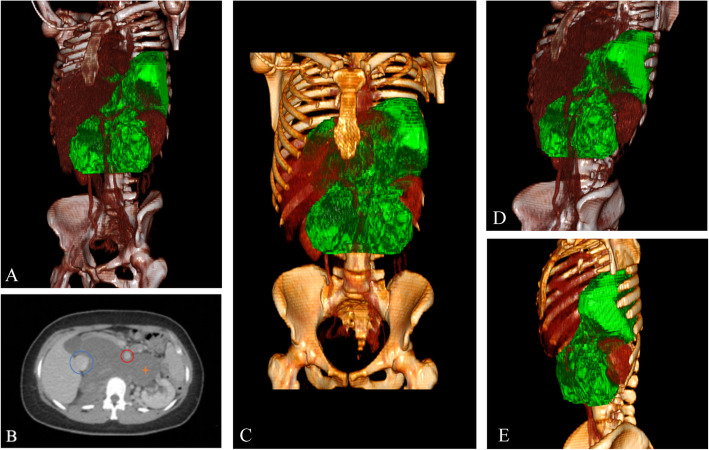
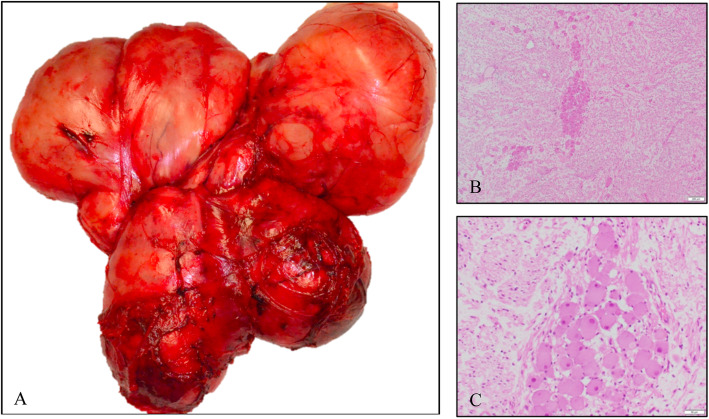
A 30-year-old female was referred to our oncologic center due to a giant retroperitoneal and mediastinal mass detected in computed tomography (CT) scans. The initial symptoms were transient nausea, diarrhea, and crampy abdominal pain. There was a positive family history including 5 first- and second-degree relatives. Presurgical biopsy revealed a benign ganglioneuroma. Total resection (TR) of a 35 × 25 × 25 cm, 2550-g tumor was obtained successfully via laparotomy combined with thoracotomy and partial incision of the diaphragm. Histopathological analysis confirmed the diagnosis. Surgically challenging aspects were the bilateral tumor invasion from the retroperitoneum into the mediastinum through the aortic hiatus with the need of a bilateral 2-cavity procedure, as well as the tumor-related displacement of the abdominal aorta, the mesenteric vessels, and the inferior vena cava. Due to their anatomic course through the tumor mass, the lumbar aortic vessels needed to be partially resected. Postoperative functioning was excellent without any sign of neurologic deficit.
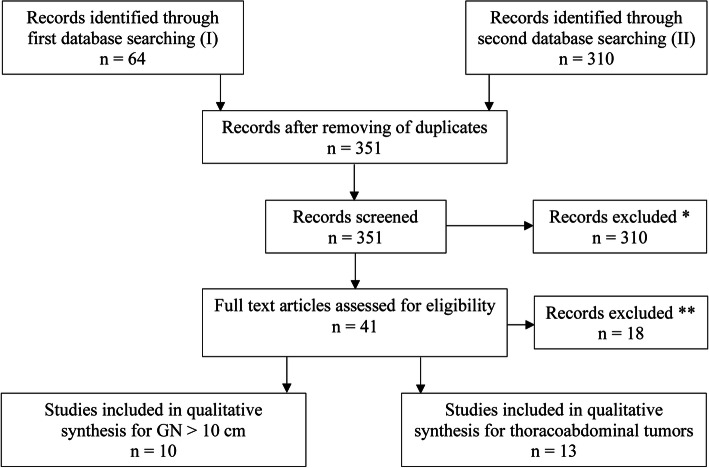
Here, we present the largest case of a TR of a GN with retroperitoneal and mediastinal expansion. On review of the literature, this is the largest reported GN resected and was performed safely. Additionally, we present the first systematic literature review for large GN (> 10 cm) as well as for resected tumors growing from the abdominal cavity into the thoracic cavity.
神经节神经瘤(GNs)极为罕见,生长缓慢,是一种可起源于施万细胞、神经节细胞以及神经元或纤维组织的良性肿瘤。因其起源于交感神经嵴,故具有神经内分泌潜能;然而,据报道大多数神经节神经瘤无激素活性。尽管如此,仍建议进行完整手术切除以控制症状或预防潜在的恶性变。
一名30岁女性因计算机断层扫描(CT)发现巨大的腹膜后和纵隔肿块被转诊至我们的肿瘤中心。最初症状为短暂的恶心、腹泻和痉挛性腹痛。有阳性家族史,包括5名一级和二级亲属。术前活检显示为良性神经节神经瘤。通过剖腹手术联合开胸手术及部分膈肌切开术,成功完整切除了一个大小为35×25×25 cm、重达2550 g的肿瘤。组织病理学分析确诊了诊断。手术面临的挑战包括肿瘤经主动脉裂孔从腹膜后双侧侵犯纵隔,需要进行双侧双腔手术,以及肿瘤导致腹主动脉、肠系膜血管和下腔静脉移位。由于腰主动脉血管在肿瘤块内的走行,需要部分切除。术后功能良好,无任何神经功能缺损迹象。
在此,我们报告了一例最大的神经节神经瘤完整切除术病例,该肿瘤累及腹膜后和纵隔。经文献检索,这是已报道的最大的神经节神经瘤切除病例,且手术安全完成。此外,我们首次对大型神经节神经瘤(>10 cm)以及从腹腔生长至胸腔的切除肿瘤进行了系统的文献综述。