Li Xiang, Xu Zhongmou, Wang Tianyi, Xu Xiang, Li Haiying, Sun Qin, Zhou Xinmin, Chen Gang
Department of Clinical Medicine, The First Affiliated Hospital of Soochow University, Suzhou, Jiangsu Province, China.
Department of Neurosurgery, The Affiliated Jiangyin Hospital, School of Medicine, Southeast University, Jiangyin, Jiangsu Province, China.
Clin Epidemiol Glob Health. 2021 Jan-Mar;9:184-190. doi: 10.1016/j.cegh.2020.08.012. Epub 2020 Sep 15.
To identify clinical characteristics of severe patients with COVID-19.
The WHO database of publications on COVID-19 and PubMed were searched from inception to March 20, 2020 and all valuable studies were analyzed using Stata 15.0.
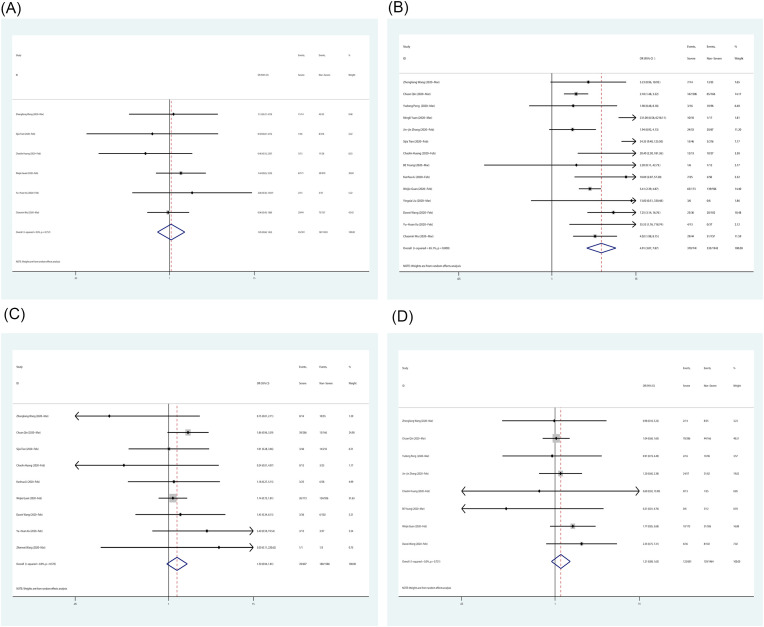
We selected forty-four studies with 13,497 patients. In the comparison of severe and non-severe groups, age over 50 (OR = 4.090; 95% CI = 2.422-6.907, P = 0.000) and underlying disease (OR = 3.992; 95% CI = 2.631-6.507, P = 0.000) are risk factors. Female gender (OR = 0.740; 95% CI = 0.622-0.881, P = 0.001) is a protective factor. Characteristics like dyspnea (OR = 4.914; 95% CI = 3.069-7.867, P = 0.000), lymphopenia (OR = 5.528; 95% CI = 3.484-8.772, P = 0.000), thrombocytopenia (OR = 3.623; 95% CI = 1.034-12.691, P = 0.044), elevated C-reactive protein (OR = 5.217; 95% CI = 2.459-11.070, P = 0.000) and D-dimer (OR = 3.780; 95% CI = 1.481-9.648, P = 0.005) were more frequently in severe cases. Diffuse lesions and consolidation (OR = 4.680; 95% CI = 3.183-6.881, P = 0.000) in imaging was considered reliable.
Men older than 50 with underlying disease are susceptible to develop severe pneumonia while female gender is protective. The typical symptom of severe pneumonia was dyspnea, but high fever, headache and diarrhea were not significantly different among patients with varying degrees of severity. Lymphopenia, thrombocytopenia, elevated C-reactive protein and D-dimer occurred more frequently in severe patients and yet leukopenia is not a characteristic laboratory indicator. Diffuse lesions and consolidation are important imaging features to distinguish severe pneumonia.
确定新型冠状病毒肺炎(COVID-19)重症患者的临床特征。
检索世界卫生组织(WHO)关于COVID-19的出版物数据库以及PubMed,检索时间从数据库建立至2020年3月20日,使用Stata 15.0对所有有价值的研究进行分析。
我们选取了44项研究,共13497例患者。在重症组与非重症组的比较中,年龄超过50岁(比值比[OR]=4.090;95%置信区间[CI]=2.422 - 6.907,P=0.000)和基础疾病(OR=3.992;95% CI=2.631 - 6.507,P=0.000)是危险因素。女性(OR=0.740;95% CI=0.622 - 0.881,P=0.001)是保护因素。呼吸困难(OR=4.914;95% CI=3.069 - 7.867,P=0.000)、淋巴细胞减少(OR=5.528;95% CI=3.484 - 8.772,P=0.000)、血小板减少(OR=3.623;95% CI=1.034 - 12.691, P=0.044)、C反应蛋白升高(OR=5.217;95% CI=2.459 - 11.070,P=0.000)和D-二聚体升高(OR=3.780;95% CI=1.481 - 9.648,P=0.005)等特征在重症病例中更常见。影像学上的弥漫性病变和实变(OR=4.680;95% CI=3.183 - 6.881,P=0.000)被认为是可靠的。
年龄超过50岁且有基础疾病的男性易发生重症肺炎,而女性具有保护作用。重症肺炎的典型症状是呼吸困难,但不同严重程度患者的高热、头痛和腹泻无显著差异。淋巴细胞减少、血小板减少、C反应蛋白升高和D-二聚体升高在重症患者中更常见,而白细胞减少不是特征性的实验室指标。弥漫性病变和实变是区分重症肺炎的重要影像学特征。