Jacobs Werner, Lammens Martin, Kerckhofs Annelies, Voets Evy, Van San Emily, Van Coillie Samya, Peleman Cédric, Mergeay Matthias, Sirimsi Sabriya, Matheeussen Veerle, Jansens Hilde, Baar Ingrid, Vanden Berghe Tom, Jorens Philippe G
Department of Forensic Medicine, Antwerp University Hospital, University of Antwerp, Edegem, Belgium.
Military Hospital Queen Astrid, Crisis Unit, Belgian Defense, Brussels, Belgium.
ESC Heart Fail. 2020 Dec;7(6):3772-3781. doi: 10.1002/ehf2.12958. Epub 2020 Sep 22.
Cardiovascular complications, including myocarditis, are observed in coronavirus disease 2019 (COVID-19). Major cardiac involvement is a potentially lethal feature in severe cases. We sought to describe the underlying pathophysiological mechanism in COVID-19 lethal cardiogenic shock.
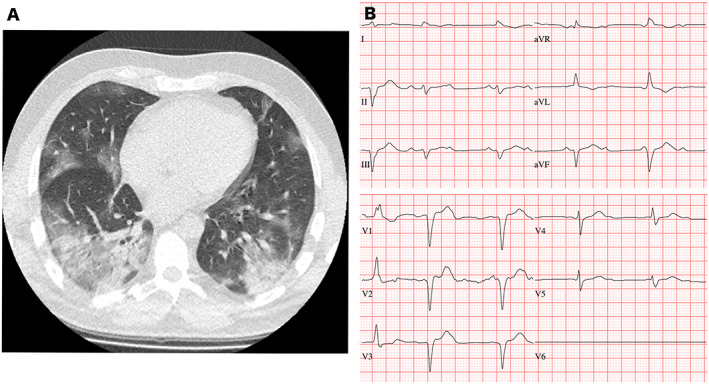
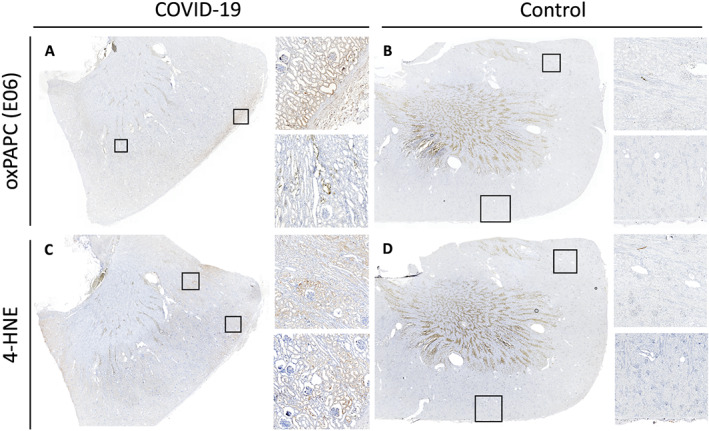
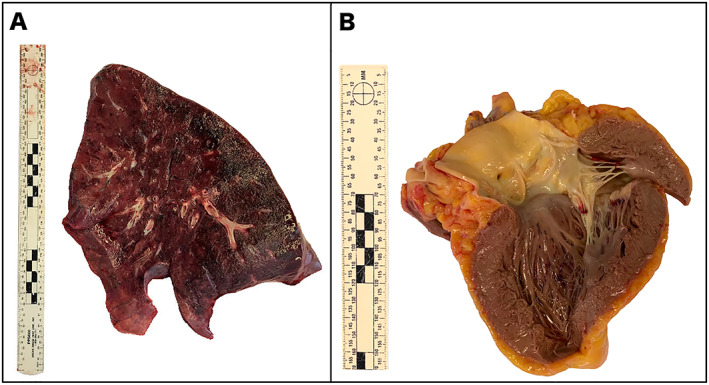
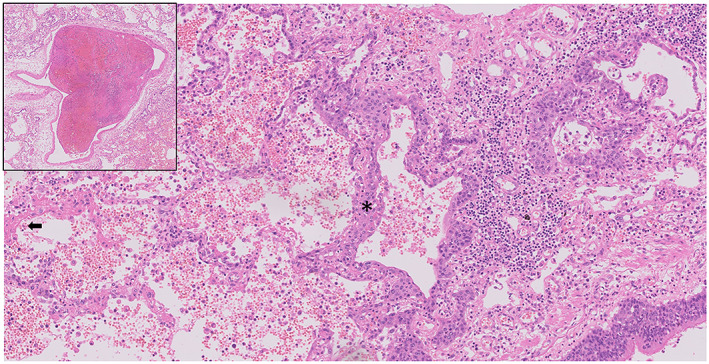
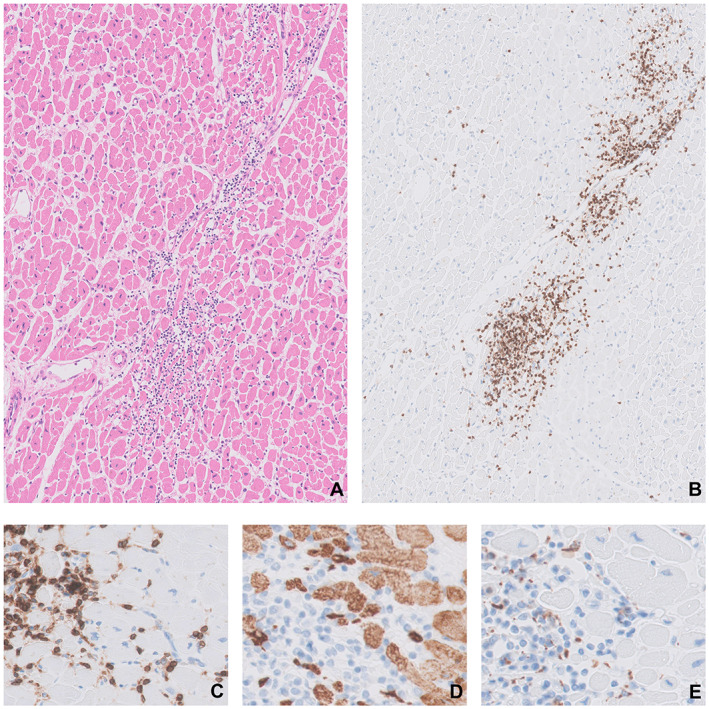
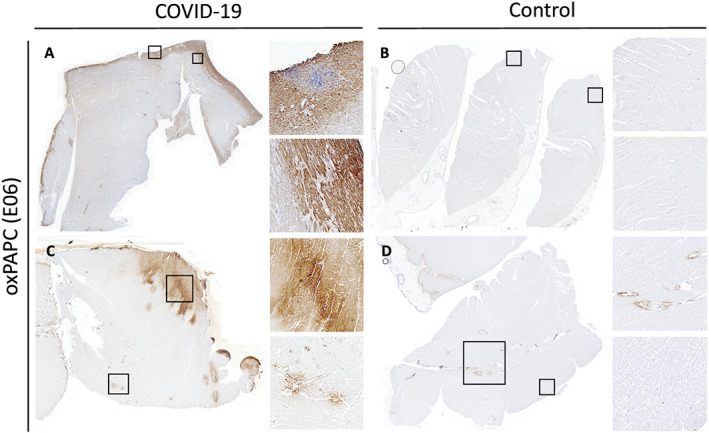
We report on a 48-year-old male COVID-19 patient with cardiogenic shock; despite extracorporeal life support, dialysis, and massive pharmacological support, this rescue therapy was not successful. Severe acute respiratory syndrome coronavirus 2 RNA was detected at autopsy in the lungs and myocardium. Histopathological examination revealed diffuse alveolar damage, proliferation of type II pneumocytes, lymphocytes in the lung interstitium, and pulmonary microemboli. Moreover, patchy muscular, sometimes perivascular, interstitial mononuclear inflammatory infiltrates, dominated by lymphocytes, were seen in the cardiac tissue. The lymphocytes 'interlocked' the myocytes, resulting in myocyte degeneration and necrosis. Predominantly, T-cell lymphocytes with a CD4:CD8 ratio of 1.7 infiltrated the interstitial myocardium, reflecting true myocarditis. The myocardial tissue was examined for markers of ferroptosis, an iron-catalysed form of regulated cell death that occurs through excessive peroxidation of polyunsaturated fatty acids. Immunohistochemical staining with E06, a monoclonal antibody binding to oxidized phosphatidylcholine (reflecting lipid peroxidation during ferroptosis), was positive in morphologically degenerating and necrotic cardiomyocytes adjacent to the infiltrate of lymphocytes, near arteries, in the epicardium and myocardium. A similar ferroptosis signature was present in the myocardium of a COVID-19 subject without myocarditis. In a case of sudden death due to viral myocarditis of unknown aetiology, however, immunohistochemical staining with E06 was negative. The renal proximal tubuli stained positively for E06 and also hydroxynonenal (4-HNE), a reactive breakdown product of the lipid peroxides that execute ferroptosis. In the case of myocarditis of other aetiology, the renal tissue displayed no positivity for E06 or 4-HNE.
The findings in this case are unique as this is the first report on accumulated oxidized phospholipids (or their breakdown products) in myocardial and renal tissue in COVID-19. This highlights ferroptosis, proposed to detrimentally contribute to some forms of ischaemia-reperfusion injury, as a detrimental factor in COVID-19 cardiac damage and multiple organ failure.
在2019冠状病毒病(COVID-19)中观察到包括心肌炎在内的心血管并发症。严重病例中主要的心脏受累是一个潜在的致命特征。我们试图描述COVID-19致死性心源性休克的潜在病理生理机制。
我们报告了一名48岁患有心源性休克的男性COVID-19患者;尽管进行了体外生命支持、透析和大量药物支持,但这种抢救治疗并未成功。尸检时在肺和心肌中检测到严重急性呼吸综合征冠状病毒2 RNA。组织病理学检查显示弥漫性肺泡损伤、II型肺泡上皮细胞增生、肺间质淋巴细胞浸润和肺微栓塞。此外,在心脏组织中可见散在的肌性、有时是血管周围的间质单核细胞炎性浸润,以淋巴细胞为主。淋巴细胞“环绕”心肌细胞,导致心肌细胞变性和坏死。主要是CD4:CD8比值为1.7的T淋巴细胞浸润间质心肌,反映了真正的心肌炎。对心肌组织进行铁死亡标志物检查,铁死亡是一种由铁催化的程序性细胞死亡形式,通过多不饱和脂肪酸的过度过氧化发生。用E06进行免疫组化染色,E06是一种与氧化磷脂酰胆碱结合的单克隆抗体(反映铁死亡期间的脂质过氧化),在淋巴细胞浸润附近、动脉周围、心外膜和心肌中形态学上变性和坏死的心肌细胞中呈阳性。在一名没有心肌炎的COVID-19患者的心肌中也存在类似的铁死亡特征。然而,在一例病因不明的病毒性心肌炎猝死病例中,用E06进行免疫组化染色为阴性。肾近端小管E06染色阳性,同时4-羟基壬烯醛(4-HNE)染色也呈阳性,4-HNE是执行铁死亡的脂质过氧化物的一种反应性分解产物。在其他病因的心肌炎病例中,肾组织E06或4-HNE染色均为阴性。
该病例的发现是独特的,因为这是关于COVID-19心肌和肾组织中积累的氧化磷脂(或其分解产物)的首次报告。这突出了铁死亡,铁死亡被认为对某些形式的缺血再灌注损伤有有害作用,是COVID-19心脏损伤和多器官功能衰竭的一个有害因素。