Peesapati Venkata Sri Ramani, Sadik Mohammad, Verma Sadhika, Attallah Marline A, Khan Safeera
Research, California Institute of Behavorial Neurosciences and Psychology, Fairfield, USA.
Internal Medicine, Manipal College of Medical Sciences, Pokhara, NPL.
Cureus. 2020 Aug 19;12(8):e9869. doi: 10.7759/cureus.9869.
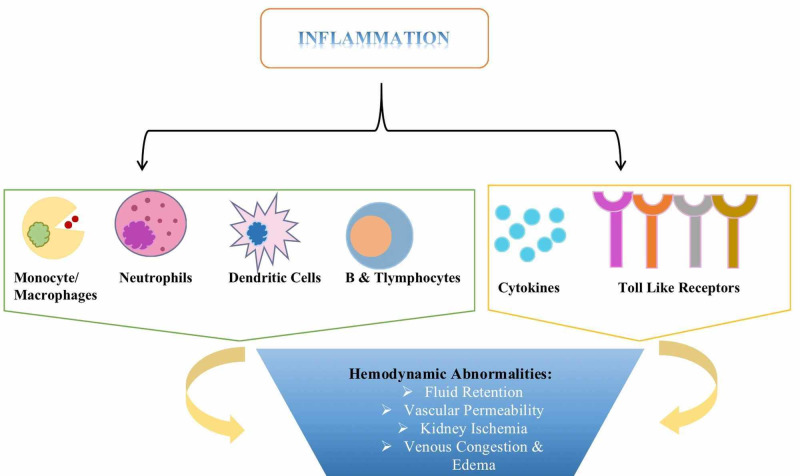
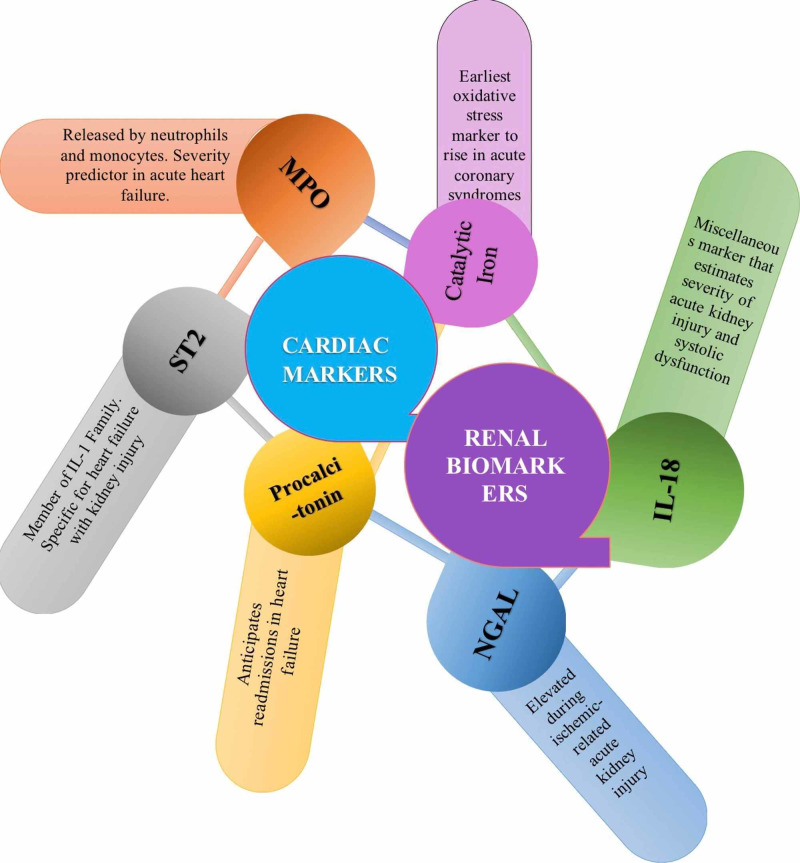
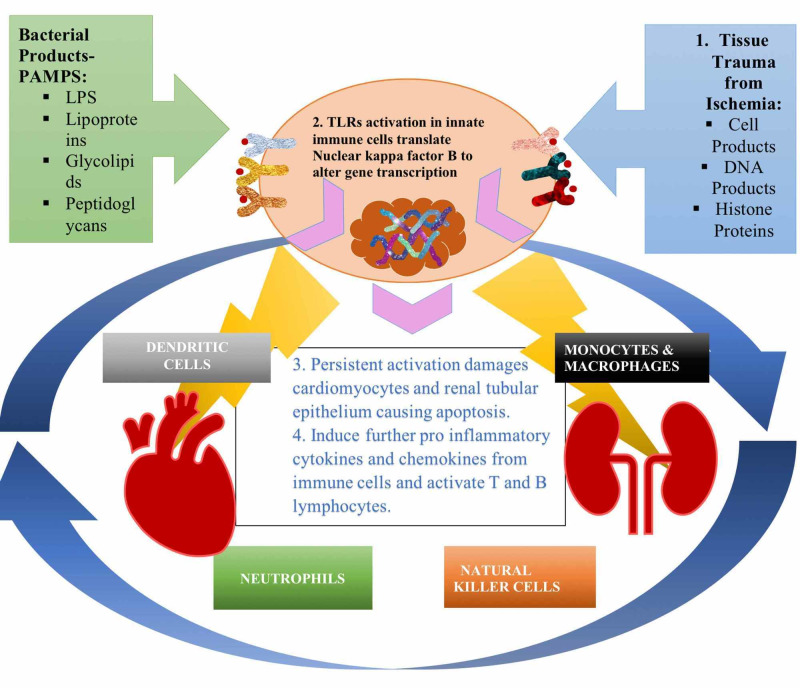
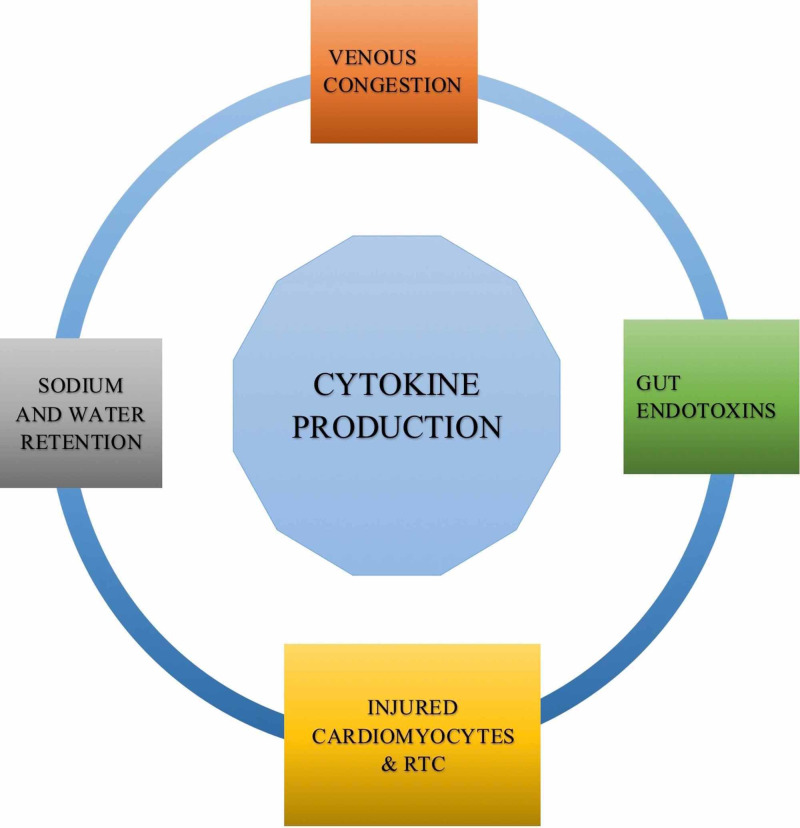
Physiological organ cross-talk is necessary to maintain equilibrium and homeostasis. Heart and kidney are the essences of this equilibrium. Organ failure in either of these organs can perturb the bidirectional communication between them, impinging this unpleasant vascular and cellular milieu on other distant organs. Cardiorenal syndrome (CRS) type I occurs due to acute deterioration of cardiac function, ultimately causing acute kidney injury (AKI). This syndrome is an intricate condition with neurohormonal and inflammatory aspects. Inflammation creates a vicious circle filled with the innate and adaptive immune systems, pro-inflammatory cytokines, chemokines to actuate hemodynamic compromise in CRS type I patients. Pro-inflammatory cytokines not only aggravate fluid retention and venous congestion but also initiate apoptosis and oxidative stress. The immune response's primary motive is to elicit the heart and kidney to produce cytokines, intensifying the inflammatory process. Despite the possible standard of care, patient mortality, treatment cost, readmissions are extreme in CRS type I, and inflammation certainly has critical inferences warranting future research in humans.
生理器官间的相互作用对于维持平衡和内稳态是必要的。心脏和肾脏是这种平衡的关键。这两个器官中任何一个发生器官衰竭都可能扰乱它们之间的双向通讯,将这种不良的血管和细胞环境影响到其他远处的器官。I型心肾综合征(CRS)是由于心脏功能急性恶化最终导致急性肾损伤(AKI)而发生的。这种综合征是一种涉及神经激素和炎症方面的复杂病症。炎症形成了一个充满先天性和适应性免疫系统、促炎细胞因子、趋化因子的恶性循环,从而在I型CRS患者中引发血流动力学损害。促炎细胞因子不仅会加重液体潴留和静脉淤血,还会引发细胞凋亡和氧化应激。免疫反应的主要目的是促使心脏和肾脏产生细胞因子,从而加剧炎症过程。尽管有可能的标准治疗方法,但I型CRS患者的死亡率、治疗成本、再入院率都极高,而且炎症肯定有重要影响,值得未来在人类身上进行研究。