Department of Obstetrics and Gynaecology, Centre of Perinatal Medicine and Health, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Södra Älvsborg Hospital, Borås, Sweden.
BJOG. 2021 Jan;128(2):195-206. doi: 10.1111/1471-0528.16519. Epub 2020 Oct 19.
To estimate the diagnostic performance of sonographic cervical length for the prediction of preterm birth (PTB).
Prospective observational multicentre study.
Seven Swedish ultrasound centres.
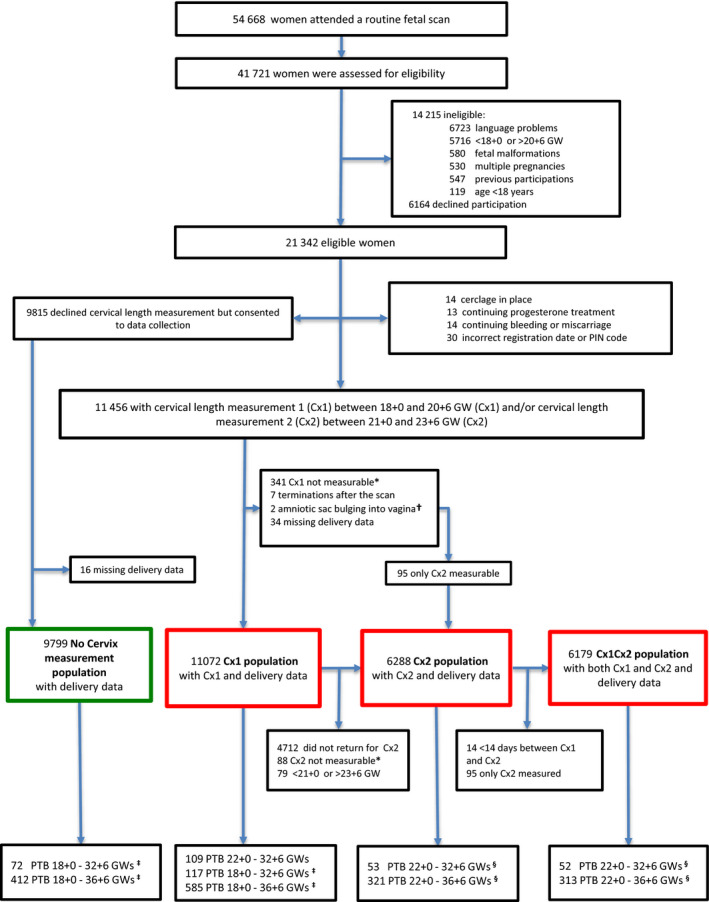
A cohort of 11 456 asymptomatic women with a singleton pregnancy.
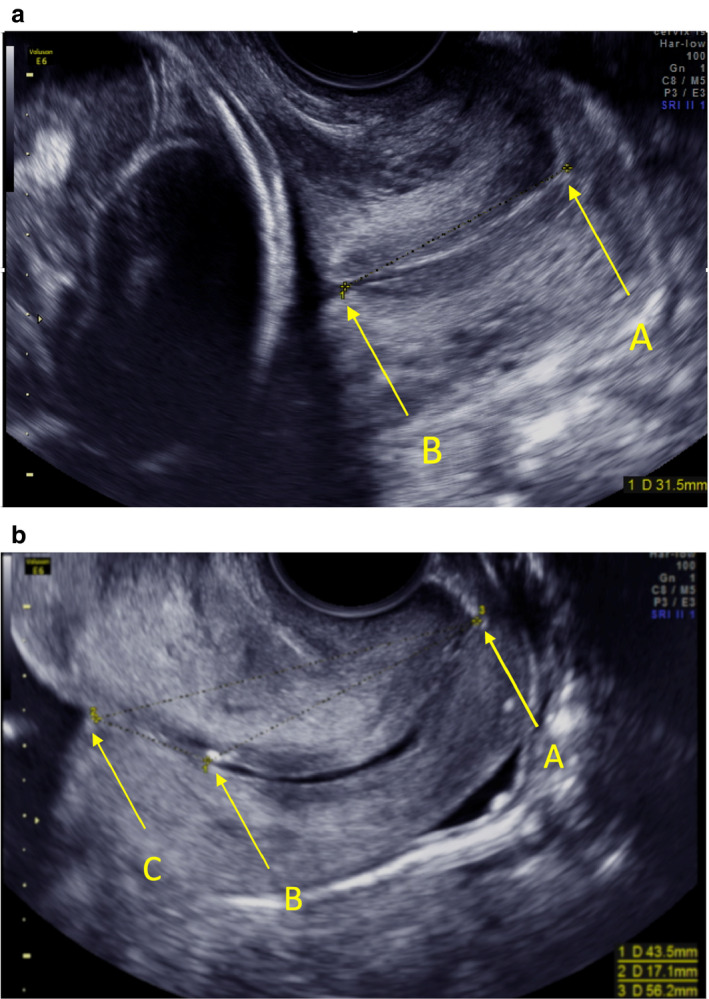
Cervical length was measured with transvaginal ultrasound at 18-20 weeks of gestation (C×1) and at 21-23 weeks of gestation (C×2, optional). Staff and participants were blinded to results.
Area under receiver operating characteristic curve (AUC), sensitivity, specificity, positive and negative predictive values (PPV and NPV), positive and negative likelihood ratios (LR+ and LR-), number of false-positive results per true-positive result (FP/TP), number needed to screen to detect one PTB (NNS) and prevalence of 'short' cervix.
Spontaneous PTB (sPTB) at <33 weeks of gestation occurred in 56/11 072 (0.5%) women in the C×1 population (89% white) and in 26/6288 (0.4%) in the C×2 population (92% white). The discriminative ability of shortest endocervical length was better the earlier the sPTB occurred and was better at C×2 than at C×1 (AUC to predict sPTB at <33 weeks of gestation 0.76 versus 0.65, difference in AUC 0.11, 95% CI 0.01-0.23). At C×2, the shortest endocervical length of ≤25 mm (prevalence 4.4%) predicted sPTB at <33 weeks of gestation with sensitivity 38.5% (10/26), specificity 95.8% (5998/6262), PPV 3.6% (10/274), NPV 99.7% (5988/6014), LR+ 9.1, LR- 0.64, FP/TP 26 and NNS 629.
Second-trimester sonographic cervical length can identify women at high risk of sPTB. In a population of mainly white women with a low prevalence of sPTB its diagnostic performance is at best moderate.
Cervical length screening to predict preterm birth in a white low-risk population has moderate performance.
评估超声宫颈长度预测早产(PTB)的诊断性能。
前瞻性观察性多中心研究。
瑞典 7 家超声中心。
11456 例无症状单胎妊娠孕妇。
经阴道超声于 18-20 周(C×1)和 21-23 周(C×2,可选)测量宫颈长度。工作人员和参与者对结果均不知情。
受试者工作特征曲线下面积(AUC)、敏感度、特异度、阳性和阴性预测值(PPV 和 NPV)、阳性和阴性似然比(LR+ 和 LR-)、每例真阳性结果的假阳性结果数(FP/TP)、每检出 1 例 PTB 所需的筛查例数(NNS)和“短”宫颈的发生率。
C×1 人群中,89%为白人,<33 孕周自发性早产(sPTB)发生率为 56/11072(0.5%);C×2 人群中,92%为白人,<33 孕周 sPTB 发生率为 26/6288(0.4%)。sPTB 发生越早,最短宫颈内口长度的鉴别能力越好,C×2 优于 C×1(预测<33 孕周 sPTB 的 AUC 为 0.76 比 0.65,AUC 差异为 0.11,95%CI 为 0.01-0.23)。在 C×2 中,最短宫颈内口长度≤25mm(发生率为 4.4%)预测<33 孕周 sPTB 的敏感度为 38.5%(10/26),特异度为 95.8%(5998/6262),PPV 为 3.6%(10/274),NPV 为 99.7%(5988/6014),LR+为 9.1,LR-为 0.64,FP/TP 为 26,NNS 为 629。
中孕期超声宫颈长度可识别 sPTB 高危孕妇。在白人低危人群中,其诊断性能最多为中等。
在白人低危人群中,筛查宫颈长度预测早产的表现为中等。