Division of Infectious Diseases, Department of Medicine, Medical College of Wisconsin, Milwaukee.
Division of General Medicine, Department of Medicine, Medical College of Wisconsin, Milwaukee.
JAMA Netw Open. 2020 Sep 1;3(9):e2021892. doi: 10.1001/jamanetworkopen.2020.21892.
Initial public health data show that Black race may be a risk factor for worse outcomes of coronavirus disease 2019 (COVID-19).
To characterize the association of race with incidence and outcomes of COVID-19, while controlling for age, sex, socioeconomic status, and comorbidities.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study included 2595 consecutive adults tested for COVID-19 from March 12 to March 31, 2020, at Froedtert Health and Medical College of Wisconsin (Milwaukee), the largest academic system in Wisconsin, with 879 inpatient beds (of which 128 are intensive care unit beds).
Race (Black vs White, Native Hawaiian or Pacific Islander, Native American or Alaska Native, Asian, or unknown).
Main outcomes included COVID-19 positivity, hospitalization, intensive care unit admission, mechanical ventilation, and death. Additional independent variables measured and tested included socioeconomic status, sex, and comorbidities. Reverse transcription polymerase chain reaction assay was used to test for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
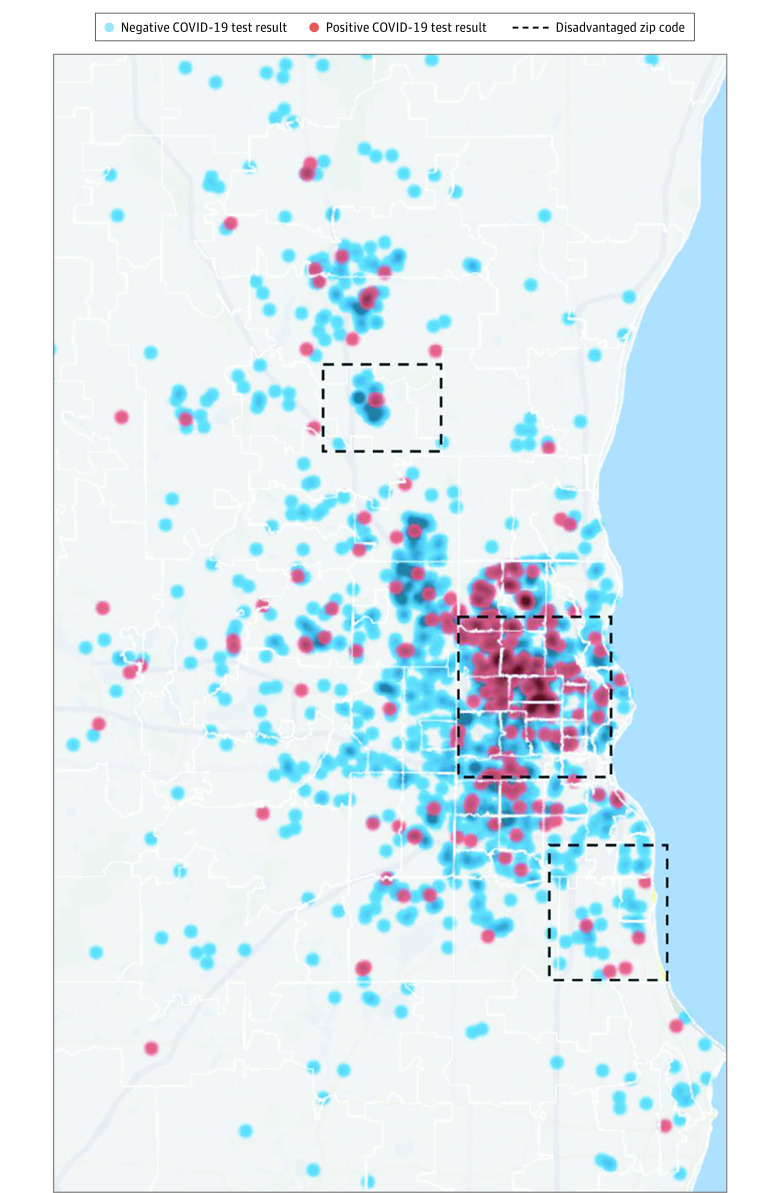
A total of 2595 patients were included. The mean (SD) age was 53.8 (17.5) years, 978 (37.7%) were men, and 785 (30.2%) were African American patients. Of the 369 patients (14.2%) who tested positive for COVID-19, 170 (46.1%) were men, 148 (40.1%) were aged 60 years or older, and 218 (59.1%) were African American individuals. Positive tests were associated with Black race (odds ratio [OR], 5.37; 95% CI, 3.94-7.29; P = .001), male sex (OR, 1.55; 95% CI, 1.21-2.00; P = .001), and age 60 years or older (OR, 2.04; 95% CI, 1.53-2.73; P = .001). Zip code of residence explained 79% of the overall variance in COVID-19 positivity in the cohort (ρ = 0.79; 95% CI, 0.58-0.91). Adjusting for zip code of residence, Black race (OR, 1.85; 95% CI, 1.00-3.65; P = .04) and poverty (OR, 3.84; 95% CI, 1.20-12.30; P = .02) were associated with hospitalization. Poverty (OR, 3.58; 95% CI, 1.08-11.80; P = .04) but not Black race (OR, 1.52; 95% CI, 0.75-3.07; P = .24) was associated with intensive care unit admission. Overall, 20 (17.2%) deaths associated with COVID-19 were reported. Shortness of breath at presentation (OR, 10.67; 95% CI, 1.52-25.54; P = .02), higher body mass index (OR per unit of body mass index, 1.19; 95% CI, 1.05-1.35; P = .006), and age 60 years or older (OR, 22.79; 95% CI, 3.38-53.81; P = .001) were associated with an increased likelihood of death.
In this cross-sectional study of adults tested for COVID-19 in a large midwestern academic health system, COVID-19 positivity was associated with Black race. Among patients with COVID-19, both race and poverty were associated with higher risk of hospitalization, but only poverty was associated with higher risk of intensive care unit admission. These findings can be helpful in targeting mitigation strategies for racial disparities in the incidence and outcomes of COVID-19.
最初的公共卫生数据表明,黑色人种可能是导致 2019 年冠状病毒病(COVID-19)结局较差的一个风险因素。
在控制年龄、性别、社会经济地位和合并症的情况下,描述种族与 COVID-19 发病和结局的关联。
设计、地点和参与者:这项横断面研究纳入了 2020 年 3 月 12 日至 3 月 31 日期间在威斯康星州密尔沃基的弗雷德特健康和威斯康星医学院(密尔沃基最大的学术系统,有 879 张住院病床(其中 128 张为重症监护病床))接受 COVID-19 检测的 2595 例连续成年患者。
种族(黑人与白人、夏威夷原住民或太平洋岛民、美洲原住民或阿拉斯加原住民、亚洲人或未知)。
主要结局包括 COVID-19 阳性、住院、入住重症监护病房、机械通气和死亡。还测量并测试了其他独立变量,包括社会经济地位、性别和合并症。使用逆转录聚合酶链反应检测严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)。
共纳入 2595 例患者。患者的平均(标准差)年龄为 53.8(17.5)岁,978 例(37.7%)为男性,785 例(30.2%)为非裔美国人。在 369 例 COVID-19 检测呈阳性的患者中,170 例(46.1%)为男性,148 例(40.1%)年龄在 60 岁或以上,218 例(59.1%)为非裔美国人。阳性检测结果与黑人种族(比值比[OR],5.37;95%置信区间[CI],3.94-7.29;P = 0.001)、男性(OR,1.55;95%CI,1.21-2.00;P = 0.001)和 60 岁或以上(OR,2.04;95%CI,1.53-2.73;P = 0.001)有关。居住邮政编码解释了队列中 COVID-19 阳性的总体方差的 79%(ρ = 0.79;95%CI,0.58-0.91)。在调整了居住邮政编码后,黑人种族(OR,1.85;95%CI,1.00-3.65;P = 0.04)和贫困(OR,3.84;95%CI,1.20-12.30;P = 0.02)与住院有关。贫困(OR,3.58;95%CI,1.08-11.80;P = 0.04)而不是黑人种族(OR,1.52;95%CI,0.75-3.07;P = 0.24)与重症监护病房入住有关。总体而言,20 例(17.2%)COVID-19 相关死亡报告。发病时出现呼吸急促(OR,10.67;95%CI,1.52-25.54;P = 0.02)、较高的体重指数(每单位体重指数的 OR,1.19;95%CI,1.05-1.35;P = 0.006)和 60 岁或以上(OR,22.79;95%CI,3.38-53.81;P = 0.001)与死亡风险增加有关。
在这项针对密尔沃基大型中西部学术健康系统中 COVID-19 检测的成年人的横断面研究中,COVID-19 阳性与黑色人种有关。在 COVID-19 患者中,种族和贫困均与住院风险增加相关,但只有贫困与入住重症监护病房的风险增加相关。这些发现有助于针对 COVID-19 发病率和结局的种族差异制定减轻策略。