Department of Infectious Diseases, Henry Ford Hospital, Detroit, Michigan.
Department of Internal Medicine, Henry Ford Hospital, Detroit, Michigan.
JAMA Netw Open. 2020 Jun 1;3(6):e2012270. doi: 10.1001/jamanetworkopen.2020.12270.
In late December 2019, an outbreak caused by a novel severe acute respiratory syndrome coronavirus 2 emerged in Wuhan, China. Data on the clinical characteristics and outcomes of infected patients in urban communities in the US are limited.
To describe the clinical characteristics and outcomes of patients with coronavirus disease 2019 (COVID-19) and to perform a comparative analysis of hospitalized and ambulatory patient populations.
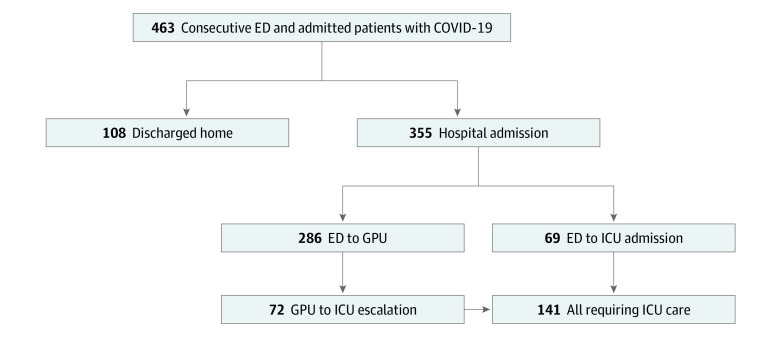
DESIGN, SETTING, AND PARTICIPANTS: This study is a case series of 463 consecutive patients with COVID-19 evaluated at Henry Ford Health System in metropolitan Detroit, Michigan, from March 9 to March 27, 2020. Data analysis was performed from March to April 2020.
Laboratory-confirmed severe acute respiratory syndrome coronavirus 2 infection.
Demographic data, underlying comorbidities, clinical presentation, complications, treatment, and outcomes were collected.
Of 463 patients with COVID-19 (mean [SD] age, 57.5 [16.8] years), 259 (55.9%) were female, and 334 (72.1%) were African American. Most patients (435 [94.0%]) had at least 1 comorbidity, including hypertension (295 patients [63.7%]), chronic kidney disease (182 patients [39.3%]), and diabetes (178 patients [38.4%]). Common symptoms at presentation were cough (347 patients [74.9%]), fever (315 patients [68.0%]), and dyspnea (282 patients [60.9%]). Three hundred fifty-five patients (76.7%) were hospitalized; 141 (39.7%) required intensive care unit management and 114 (80.8%) of those patients required invasive mechanical ventilation. Male sex (odds ratio [OR], 2.0; 95% CI, 1.3-3.2; P = .001), severe obesity (OR, 2.0; 95% CI, 1.4-3.6; P = .02), and chronic kidney disease (OR, 2.0; 95% CI, 1.3-3.3; P = .006) were independently associated with intensive care unit admission. Patients admitted to the intensive care unit had longer length of stay and higher incidence of respiratory failure and acute respiratory distress syndrome requiring invasive mechanical ventilation, acute kidney injury requiring dialysis, shock, and mortality (57 patients [40.4%] vs 15 patients [7.0%]) compared with patients in the general practice unit. Twenty-nine (11.2%) of those discharged from the hospital were readmitted and, overall, 20.0% died within 30 days. Male sex (OR, 1.8; 95% CI, 1.1-3.1; P = .03) and age older than 60 years (OR, 5.3; 95% CI, 2.9-9.7; P < .001) were significantly associated with mortality, whereas African American race was not (OR, 0.98; 95% CI, 0.54-1.8; P = .86).
In this review of urban metropolitan patients with COVID-19, most were African American with a high prevalence of comorbid conditions and high rates of hospitalization, intensive care unit admission, complications, and mortality due to COVID-19.
2019 年 12 月下旬,一种新型严重急性呼吸综合征冠状病毒 2 在武汉市爆发。美国城市社区感染患者的临床特征和结局数据有限。
描述 2019 年冠状病毒病(COVID-19)患者的临床特征和结局,并对住院和门诊患者人群进行比较分析。
设计、地点和参与者:本研究是对 2020 年 3 月 9 日至 3 月 27 日在密歇根州底特律市亨利福特卫生系统评估的 463 例连续 COVID-19 患者的病例系列研究。数据分析于 2020 年 3 月至 4 月进行。
实验室确认的严重急性呼吸综合征冠状病毒 2 感染。
收集人口统计学数据、潜在合并症、临床表现、并发症、治疗和结局。
在 463 例 COVID-19 患者中(平均[标准差]年龄,57.5[16.8]岁),259 例(55.9%)为女性,334 例(72.1%)为非裔美国人。大多数患者(435 例[94.0%])至少有 1 种合并症,包括高血压(295 例[63.7%])、慢性肾脏病(182 例[39.3%])和糖尿病(178 例[38.4%])。常见的首发症状为咳嗽(347 例[74.9%])、发热(315 例[68.0%])和呼吸困难(282 例[60.9%])。355 例(76.7%)患者住院治疗;141 例(39.7%)需要重症监护病房管理,其中 114 例(80.8%)需要有创机械通气。男性(比值比[OR],2.0;95%置信区间[CI],1.3-3.2;P=0.001)、严重肥胖(OR,2.0;95%CI,1.4-3.6;P=0.02)和慢性肾脏病(OR,2.0;95%CI,1.3-3.3;P=0.006)与重症监护病房入院独立相关。入住重症监护病房的患者住院时间较长,呼吸衰竭和需要有创机械通气的急性呼吸窘迫综合征、需要透析的急性肾损伤、休克和死亡率较高(57 例[40.4%]比 15 例[7.0%]),与普通病房患者相比。29 例(11.2%)出院后再次入院,总体而言,30 天内有 20.0%的患者死亡。男性(OR,1.8;95%CI,1.1-3.1;P=0.03)和年龄大于 60 岁(OR,5.3;95%CI,2.9-9.7;P<0.001)与死亡率显著相关,而非裔美国人种族则无显著相关性(OR,0.98;95%CI,0.54-1.8;P=0.86)。
在对城市大都市地区 COVID-19 患者的回顾性研究中,大多数患者为非裔美国人,合并症患病率高,住院、入住重症监护病房、并发症和 COVID-19 导致的死亡率高。