Centre of Research Excellence in Translating Nutritional Science to Good Health, University of Adelaide, Adelaide, South Australia, Australia.
Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts, USA.
Diabetes Obes Metab. 2021 Jan;23(1):136-146. doi: 10.1111/dom.14202. Epub 2020 Oct 22.
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are the recommended first injectable therapy in type 2 diabetes. However, long-term persistence is suboptimal and partly attributable to gastrointestinal tolerability, particularly during initiation/escalation. Gradual titration of fixed-ratio combination GLP-1 RA/insulin therapies may improve GLP-1 RA gastrointestinal tolerability. We compared gastrointestinal adverse event (AE) rates for iGlarLixi versus GLP-1 RAs during the first 12 weeks of therapy, including a sensitivity analysis with IDegLira.
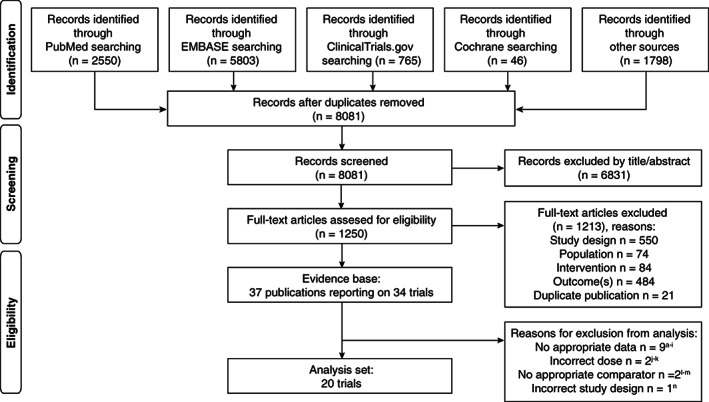
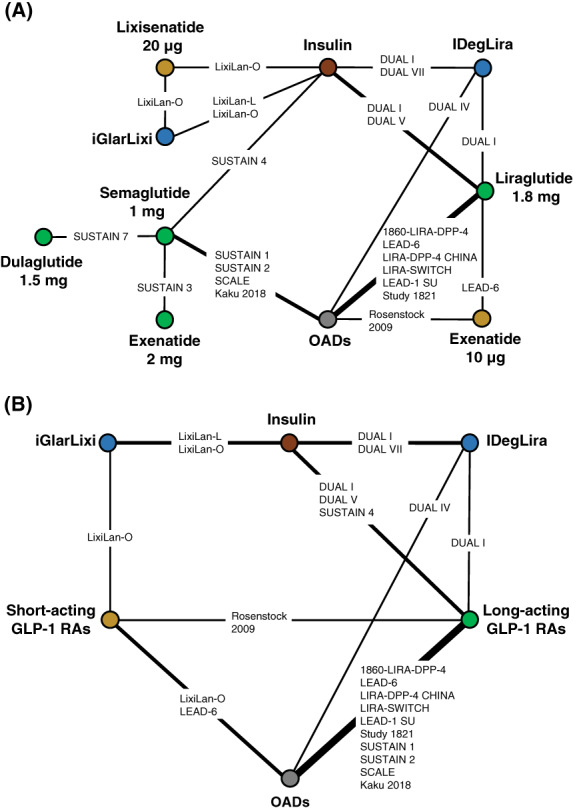
The PICO framework was used to identify studies from MEDLINE, EMBASE and CENTRAL searches using a proprietary, web-based, standardized tool with single data extraction. Gastrointestinal AEs were modelled using a Bayesian network meta-analysis (NMA), using fixed and random effects for each recommended dose (treatment-specific NMA) and class (drug-class NMA).
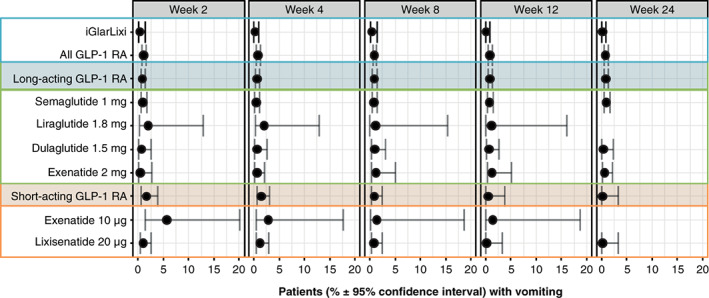
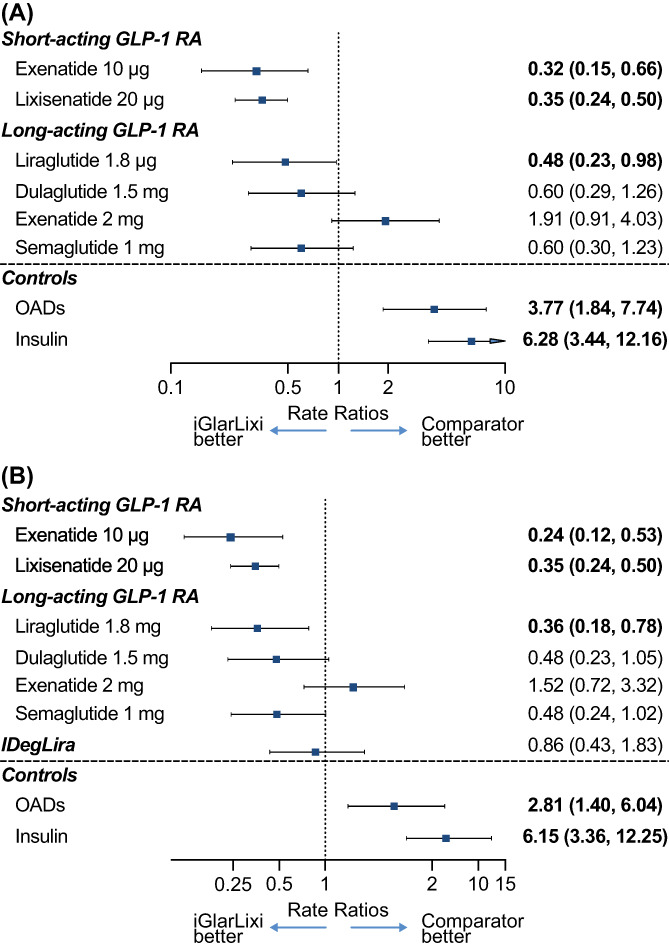
Treatment-specific NMA included 17 trials (n = 9030; 3665 event-weeks). Nausea rates were significantly lower with iGlarLixi versus exenatide 10 μg twice daily (rate ratio: 0.32; 95% credible interval: 0.15, 0.66), once-daily lixisenatide 20 μg (0.35; 0.24, 0.50) and liraglutide 1.8 mg once daily (0.48; 0.23, 0.98). Rates were numerically, but not statistically, lower versus once-weekly semaglutide 1 mg (0.60; 0.30, 1.23) and dulaglutide 1.5 mg (0.60; 0.29, 1.26), and numerically, but not statistically, higher versus once-weekly exenatide (1.91; 0.91, 4.03). Sensitivity analysis results were similar. In a naïve, pooled analysis, vomiting was lower with iGlarLixi versus other GLP-1 RAs.
During the first 12 weeks of treatment, iGlarLixi was generally associated with less nausea and vomiting than single-agent GLP-1 RAs. Enhanced gastrointestinal tolerability with fixed-ratio combinations may favour treatment persistence.
胰高血糖素样肽-1 受体激动剂(GLP-1 RAs)是 2 型糖尿病的首选注射治疗药物。然而,长期坚持治疗的情况并不理想,部分原因是胃肠道耐受性,尤其是在起始/递增阶段。固定比例联合 GLP-1 RA/胰岛素治疗的逐渐滴定可能会改善 GLP-1 RA 的胃肠道耐受性。我们比较了在治疗的前 12 周内,iGlarLixi 与 GLP-1 RA 之间胃肠道不良事件(AE)的发生率,包括使用 IDegLira 进行的敏感性分析。
使用专有、基于网络的标准化工具,通过 MEDLINE、EMBASE 和 CENTRAL 搜索,根据 PICO 框架识别研究,该工具具有单一的数据提取功能。使用贝叶斯网络荟萃分析(NMA)对胃肠道 AE 进行建模,对每个推荐剂量(治疗特异性 NMA)和类别(药物类别 NMA)使用固定和随机效应。
治疗特异性 NMA 包括 17 项试验(n = 9030;3665 个事件周)。与艾塞那肽 10 μg 每日两次(比值比:0.32;95%可信区间:0.15,0.66)、每日一次利西那肽 20μg(0.35;0.24,0.50)和每日一次利拉鲁肽 1.8mg 相比,iGlarLixi 治疗组的恶心发生率显著降低。0.48;0.23,0.98)。与每周一次的司美格鲁肽 1mg(0.60;0.30,1.23)和度拉糖肽 1.5mg(0.60;0.29,1.26)相比,率呈数值降低但无统计学意义,与每周一次的艾塞那肽(1.91;0.91,4.03)相比,率呈数值升高但无统计学意义。敏感性分析结果相似。在一项未经治疗的汇总分析中,iGlarLixi 治疗组的呕吐发生率低于其他 GLP-1 RA。
在治疗的前 12 周内,与单药 GLP-1 RA 相比,iGlarLixi 通常与较少的恶心和呕吐相关。固定比例联合治疗可提高胃肠道耐受性,从而有利于治疗的持续进行。