Jiang Yunxing, Ma Rulin, Guo Heng, Zhang Xianghui, Wang Xinping, Wang Kui, Hu Yunhua, Keerman Mulatibieke, Yan Yizhong, Ma Jiaolong, Song Yanpeng, Zhang Jingyu, He Jia, Guo Shuxia
Department of Public Health, Shihezi University School of Medicine, North 2th Road, Shihezi, Xinjiang, 832000, China.
The First Affiliated Hospital of Shihezi University Medical College, Shihezi, Xinjiang, 832000, China.
BMC Public Health. 2020 Sep 29;20(1):1471. doi: 10.1186/s12889-020-09579-4.
To externally validate the Prediction for ASCVD Risk in China (PAR) risk equation for predicting the 5-year atherosclerotic cardiovascular disease (ASCVD) risk in the Uyghur and Kazakh populations from rural areas in northwestern China and compare its performance with those of the pooled cohort equations (PCE) and Framingham risk score (FRS).
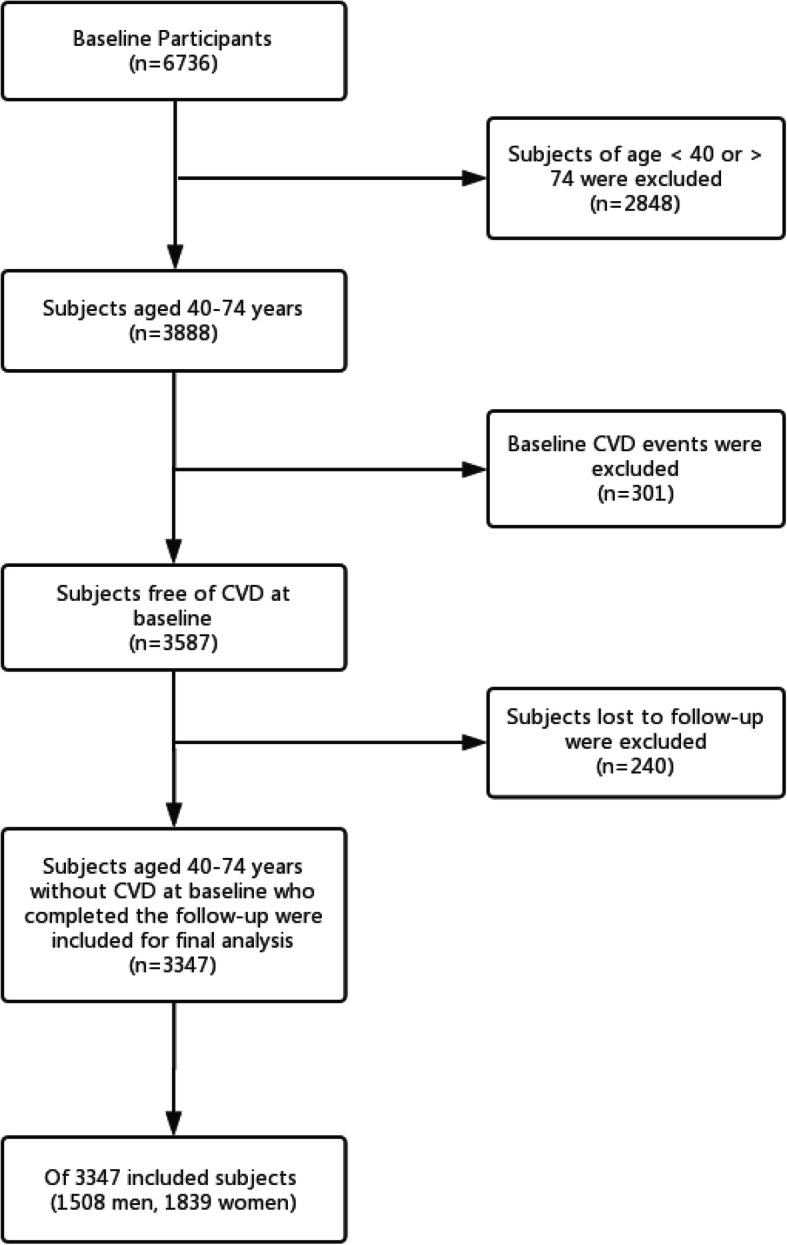
The final analysis included 3347 subjects aged 40-74 years without CVD at baseline. The 5-year ASCVD risk was calculated using the PAR, PCE, and FRS. Discrimination, calibration, and clinical usefulness of the three equations in predicting the 5-year ASCVD risk were assessed before and after recalibration.
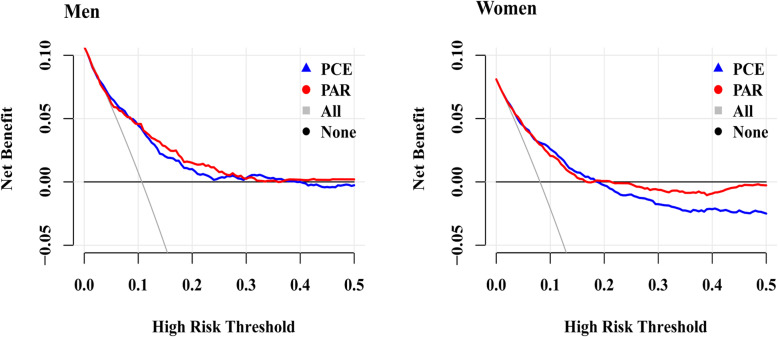
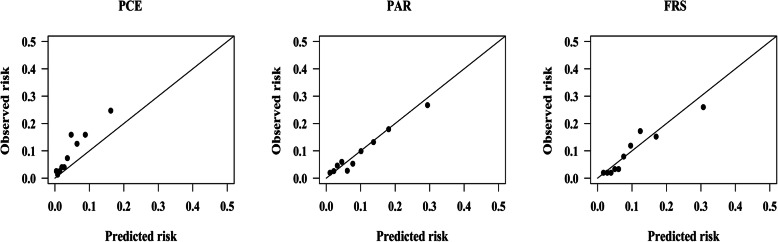
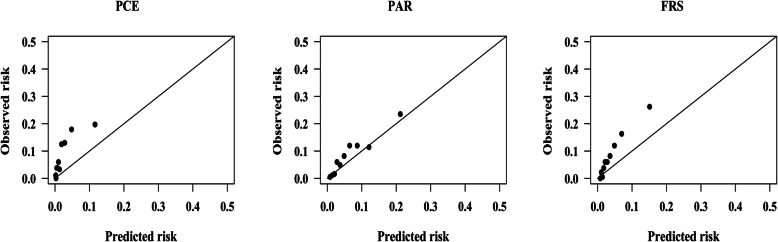
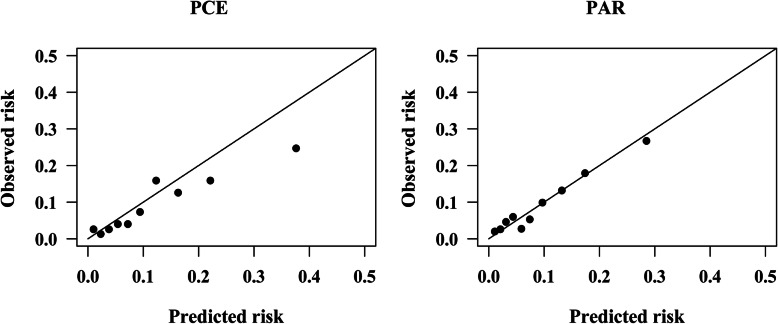
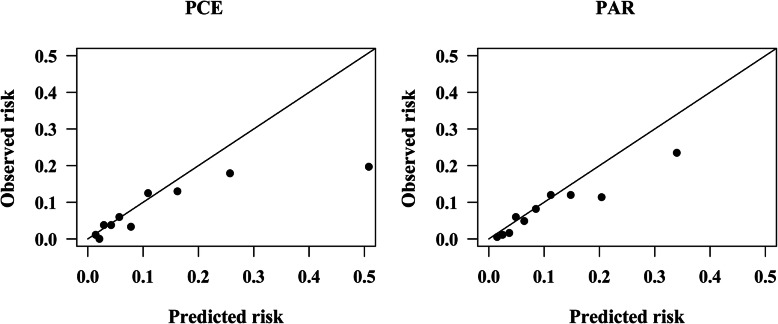
Of 3347 included subjects, 1839 were female. We observed 286 ASCVD events in within 5-year follow-up. All three risk equations had moderate discrimination in both men and women. C-indices of PAR, PCE, and FRS were 0.727 (95% CI, 0.725-0.729), 0.727 (95% CI, 0.725-0.729), and 0.740 (95% CI, 0.738-0.742), respectively, in men; the corresponding C-indices were 0.738 (95% CI, 0.737-0.739), 0.731 (95% CI, 0.730-0.732), and 0.761 (95% CI, 0.760-0.762), respectively, in women. PCE, PAR and FRS substantially underestimated the 5-year ASCVD risk in women by 70, 23 and 51%, respectively. However, PAR and FRS fairly predicted the risk in men and PAR was well calibrated. The calibrations of the three risk equations could be changed by recalibration. The decision curve analyses demonstrated that at the threshold risk of 5%, PCE was the most clinically useful in both men and women after recalibration.
All three risk equations underestimated the 5-year ASCVD risk in women, while PAR and FRS fairly predicted that in men. However, the results of predictive performances for three risk equations are inconsistent, more accurate risk equations are required in the primary prevention of ASCVD aiming to this Uyghur and Kazakh populations.
对外验证中国动脉粥样硬化性心血管疾病(ASCVD)风险预测(PAR)风险方程,以预测中国西北部农村地区维吾尔族和哈萨克族人群的5年ASCVD风险,并将其性能与汇总队列方程(PCE)和弗雷明汉风险评分(FRS)进行比较。
最终分析纳入3347名基线时无心血管疾病(CVD)的40 - 74岁受试者。使用PAR、PCE和FRS计算5年ASCVD风险。在重新校准前后评估这三个方程在预测5年ASCVD风险方面的区分度、校准度和临床实用性。
在纳入的3347名受试者中,1839名是女性。在5年随访期间观察到286例ASCVD事件。所有三个风险方程在男性和女性中均具有中等区分度。PAR、PCE和FRS在男性中的C指数分别为0.727(95%CI,0.725 - 0.729)、0.727(95%CI,0.725 - 0.729)和0.740(95%CI,0.738 - 0.742);在女性中相应的C指数分别为0.738(95%CI,0.737 - 0.739)、0.731(95%CI,0.730 - 0.732)和0.761(95%CI,0.760 - 0.762)。PCE、PAR和FRS分别将女性的5年ASCVD风险低估了70%、23%和51%。然而,PAR和FRS对男性风险的预测较为准确,且PAR校准良好。重新校准可改变这三个风险方程的校准度。决策曲线分析表明,在校准后,在5%的阈值风险下,PCE在男性和女性中临床实用性最高。
所有三个风险方程均低估了女性的5年ASCVD风险,而PAR和FRS对男性风险的预测较为准确。然而,三个风险方程的预测性能结果不一致,针对维吾尔族和哈萨克族人群的ASCVD一级预防需要更准确的风险方程。