School of Public Health, Imperial College London, London, UK.
British Pregnancy Advisory Service, London, UK.
Global Health. 2020 Sep 30;16(1):91. doi: 10.1186/s12992-020-00613-z.
In the UK, according to the 1967 Abortion Act, all abortions must be approved by two doctors, reported to the Department of Health and Social Care (DHSC), and be performed by doctors within licensed premises. Removing abortion from the criminal framework could permit new service delivery models. We explore service delivery models in primary care settings that can improve accessibility without negatively impacting the safety and efficiency of abortion services. Novel service delivery models are common in low-and-middle income countries (LMICs) due to resource constraints, and services are sometimes provided by trained, mid-level providers via "task-shifting". The aim of this study is to explore the quality of early abortion services provided in primary care of LMICs and explore the potential benefits of extending their application to the UK context.
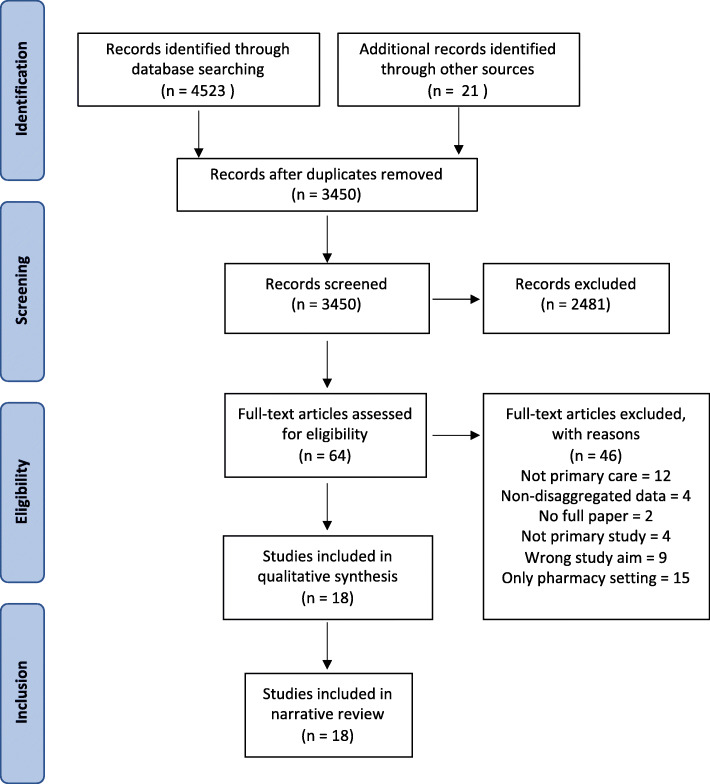
We searched MEDLINE, EMBASE, Global Health, Maternity and Infant Care, CINAHL, and HMIC for studies published from September 1994 to February 2020, with search terms "nurses", "midwives", "general physicians", "early medical/surgical abortion". We included studies that examined the quality of abortion care in primary care settings of low-and-middle-income countries (LMICs), and excluded studies in countries where abortion is illegal, and those of services provided by independent NGOs. We conducted a thematic analysis and narrative synthesis to identify indicators of quality care at structural, process and outcome levels of the Donabedian model.
A total of 21 indicators under 8 subthemes were identified to examine the quality of service provision: law and policy, infrastructure, technical competency, information provision, client-provider interactions, ancillary services, complete abortions, client satisfaction. Our analysis suggests that structural, process and outcome indicators follow a mediation pathway of the Donabedian model. This review showed that providing early medical abortion in primary care services is safe and feasible and "task-shifting" to mid-level providers can effectively replace doctors in providing abortion.
The way services are organised in LMICs, using a task-shifted and decentralised model, results in high quality services that should be considered for adoption in the UK. Collaboration with professional medical bodies and governmental departments is necessary to expand services from secondary to primary care.
在英国,根据 1967 年《堕胎法案》,所有堕胎都必须由两名医生批准,向卫生和社会保障部报告,并由持照场所内的医生进行。将堕胎从刑事框架中移除可能会允许新的服务提供模式。我们探讨了在初级保健环境中可以提高可及性而又不会对堕胎服务的安全性和效率产生负面影响的服务提供模式。由于资源限制,在中低收入国家(LMICs)中常见采用新的服务提供模式,并且有时通过“任务转移”由经过培训的中级提供者提供服务。本研究的目的是探讨在 LMICs 的初级保健中提供早期堕胎服务的质量,并探讨将其应用于英国背景的潜在益处。
我们在 MEDLINE、EMBASE、全球健康、母婴保健、CINAHL 和 HMIC 中搜索了 1994 年 9 月至 2020 年 2 月发表的研究,使用的检索词是“护士”、“助产士”、“全科医生”、“早期医疗/手术堕胎”。我们纳入了在中低收入国家(LMICs)的初级保健环境中检查堕胎护理质量的研究,排除了在堕胎非法的国家以及由独立非政府组织提供的服务的研究。我们进行了主题分析和叙述性综合,以确定在 Donabedian 模型的结构、过程和结果水平下的护理质量指标。
共确定了 21 项指标和 8 个子主题,以检查服务提供的质量:法律和政策、基础设施、技术能力、信息提供、医患互动、辅助服务、完全流产、患者满意度。我们的分析表明,结构、过程和结果指标遵循 Donabedian 模型的中介途径。这项审查表明,在初级保健服务中提供早期药物流产是安全且可行的,并且将任务转移给中级提供者可以有效地替代医生提供堕胎。
LMICs 中组织服务的方式采用任务转移和分散模式,可提供高质量的服务,应考虑在英国采用。与专业医疗机构和政府部门合作对于将服务从二级医疗扩展到初级保健是必要的。