Internal Medicine Department, Beaumont Health, Royal Oak, MI, USA.
Oakland University William Beaumont School of Medicine, Rochester, MI, USA.
Ann Med. 2021 Dec;53(1):78-86. doi: 10.1080/07853890.2020.1828616. Epub 2020 Oct 9.
Identification of patients with novel coronavirus disease 2019 (COVID-19) requiring hospital admission or at high-risk of in-hospital mortality is essential to guide patient triage and to provide timely treatment for higher risk hospitalized patients.
A retrospective multi-centre (8 hospital) cohort at Beaumont Health, Michigan, USA, reporting on COVID-19 patients diagnosed between 1 March and 1 April 2020 was used for score validation. The COVID-19 Risk of Complications Score was automatically computed by the EHR. Multivariate logistic regression models were built to predict hospital admission and in-hospital mortality using individual variables constituting the score. Validation was performed using both discrimination and calibration.
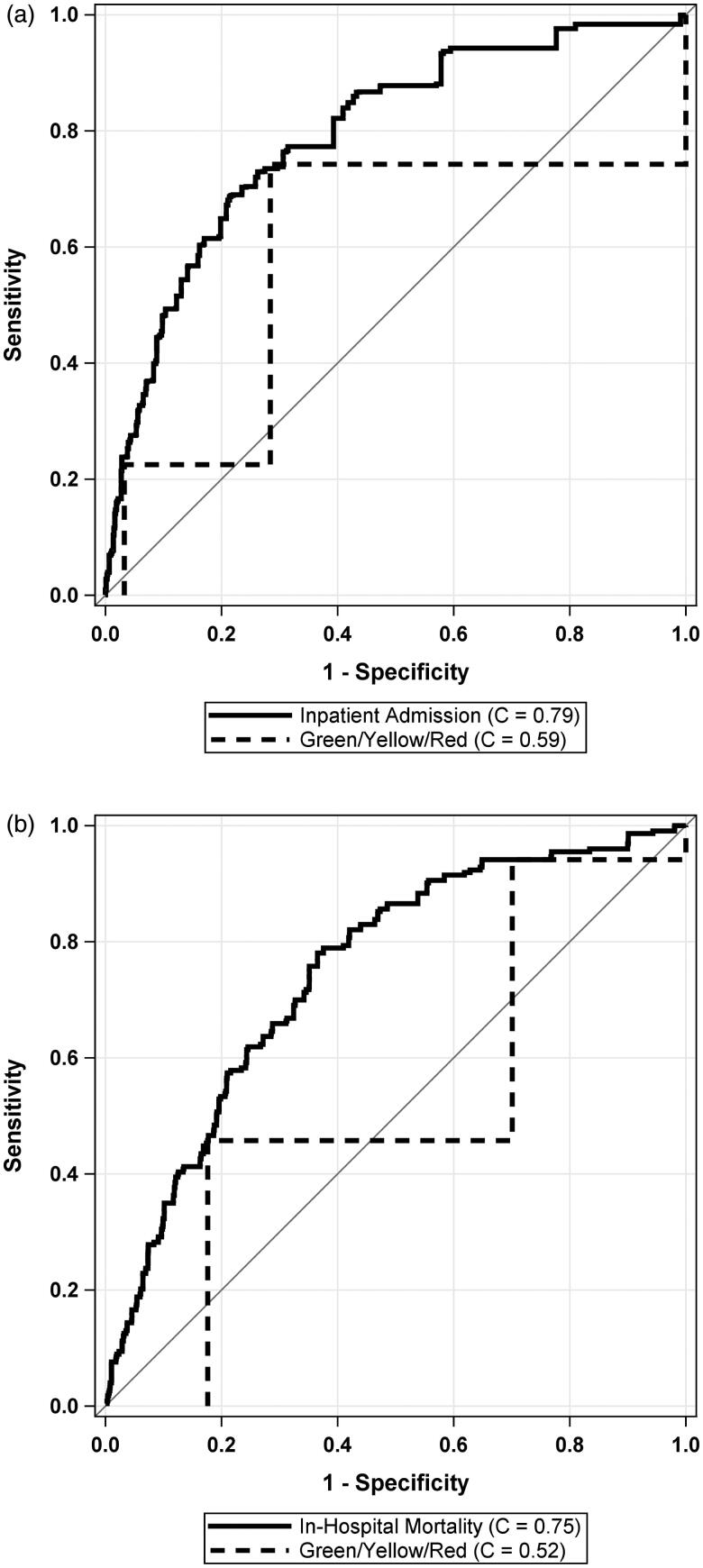
Compared to Green scores, Yellow Scores (OR: 5.72) and Red Scores (OR: 19.1) had significantly higher odds of admission (both < .0001). Similarly, Yellow Scores (OR: 4.73) and Red Scores (OR: 13.3) had significantly higher odds of in-hospital mortality than Green Scores (both < .0001). The cross-validated C-Statistics for the external validation cohort showed good discrimination for both hospital admission ( = 0.79 (95% CI: 0.77-0.81)) and in-hospital mortality ( = 0.75 (95% CI: 0.71-0.78)).
The COVID-19 Risk of Complications Score predicts the need for hospital admission and in-hospital mortality patients with COVID-19. Key points: Can an electronic health record generated risk score predict the risk of hospital admission and in-hospital mortality in patients diagnosed with coronavirus disease 2019 (COVID-19)? In both validation cohorts of 2,025 and 1,290 COVID-19, the cross-validated C-Statistics showed good discrimination for both hospital admission (C = 0.79 (95% CI: 0.77-0.81)) and in-hospital mortality (C = 0.75 (95% CI: 0.71-0.78)), respectively. The COVID-19 Risk of Complications Score may help predict the need for hospital admission if a patient contracts SARS-CoV-2 infection and in-hospital mortality for a hospitalized patient with COVID-19.
识别需要住院或有院内高死亡率风险的新型冠状病毒病 2019(COVID-19)患者对于指导患者分诊和为高风险住院患者及时治疗至关重要。
美国密歇根州 Beaumont Health 的一项回顾性多中心(8 家医院)队列研究报告了 2020 年 3 月 1 日至 4 月 1 日期间确诊的 COVID-19 患者,用于评分验证。COVID-19 并发症风险评分由电子病历自动计算。使用构成评分的个体变量构建预测住院和院内死亡率的多变量逻辑回归模型。使用判别和校准进行验证。
与 Green 评分相比,Yellow 评分(OR:5.72)和 Red 评分(OR:19.1)的住院可能性显著更高(均 < .0001)。同样,Yellow 评分(OR:4.73)和 Red 评分(OR:13.3)的院内死亡率也显著高于 Green 评分(均 < .0001)。外部验证队列的交叉验证 C-统计量显示,住院和院内死亡率的判别能力均较好(分别为 = 0.79(95%CI:0.77-0.81)和 = 0.75(95%CI:0.71-0.78))。
COVID-19 并发症风险评分可预测 COVID-19 患者住院和院内死亡的需求。
电子病历生成的风险评分能否预测冠状病毒病 2019(COVID-19)患者住院和院内死亡的风险?在 2025 例和 1290 例 COVID-19 的两个验证队列中,交叉验证的 C 统计量显示,住院(C=0.79(95%CI:0.77-0.81))和院内死亡率(C=0.75(95%CI:0.71-0.78))的判别能力均较好。COVID-19 并发症风险评分可能有助于预测 SARS-CoV-2 感染患者的住院需求和 COVID-19 住院患者的院内死亡率。