VA Connecticut Healthcare System, U.S. Department of Veterans Affairs, West Haven, Connecticut, United States of America.
Department of Neurosurgery, Yale School of Medicine, New Haven, Connecticut, United States of America.
PLoS One. 2020 Nov 11;15(11):e0241825. doi: 10.1371/journal.pone.0241825. eCollection 2020.
Available COVID-19 mortality indices are limited to acute inpatient data. Using nationwide medical administrative data available prior to SARS-CoV-2 infection from the US Veterans Health Administration (VA), we developed the VA COVID-19 (VACO) 30-day mortality index and validated the index in two independent, prospective samples.
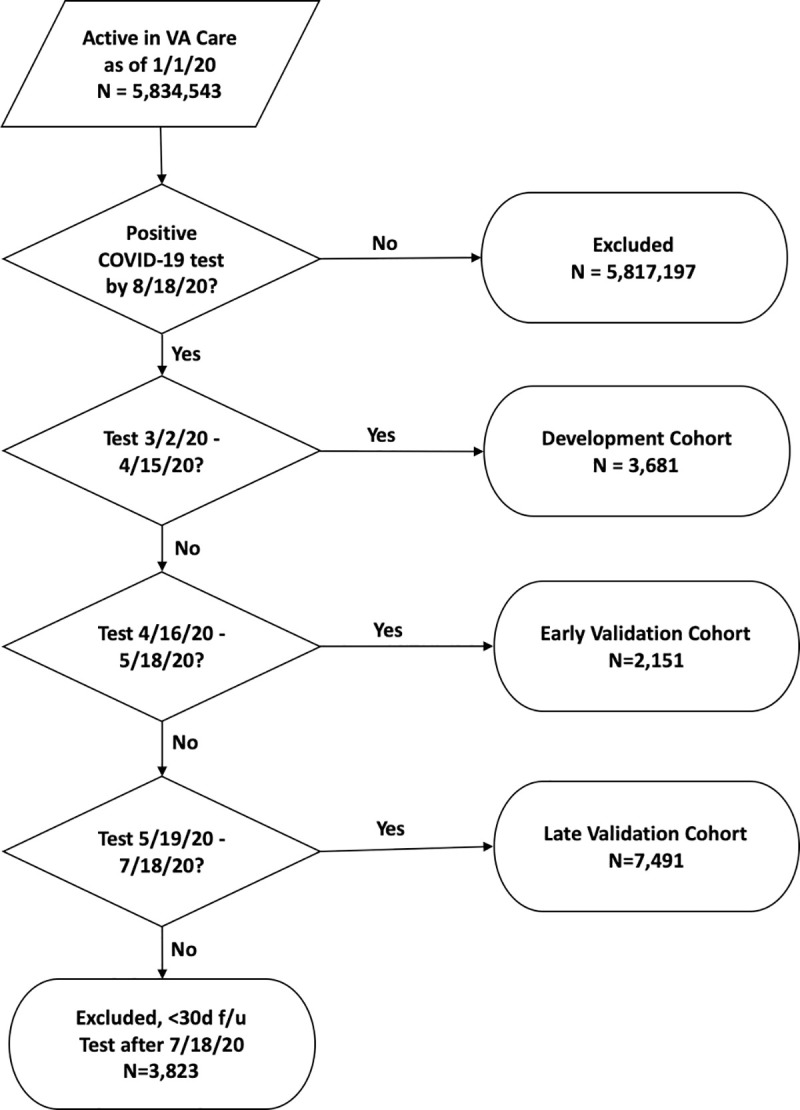
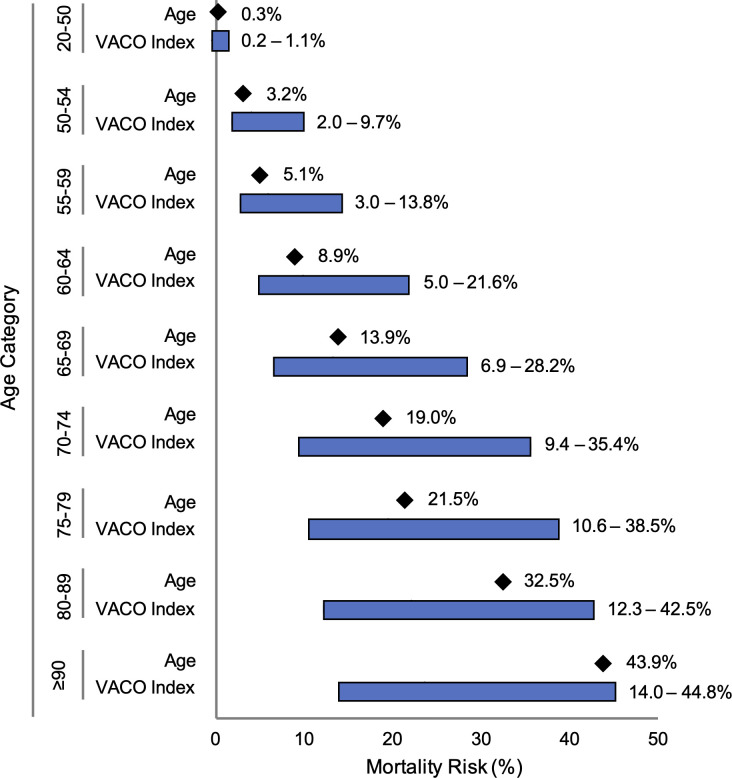
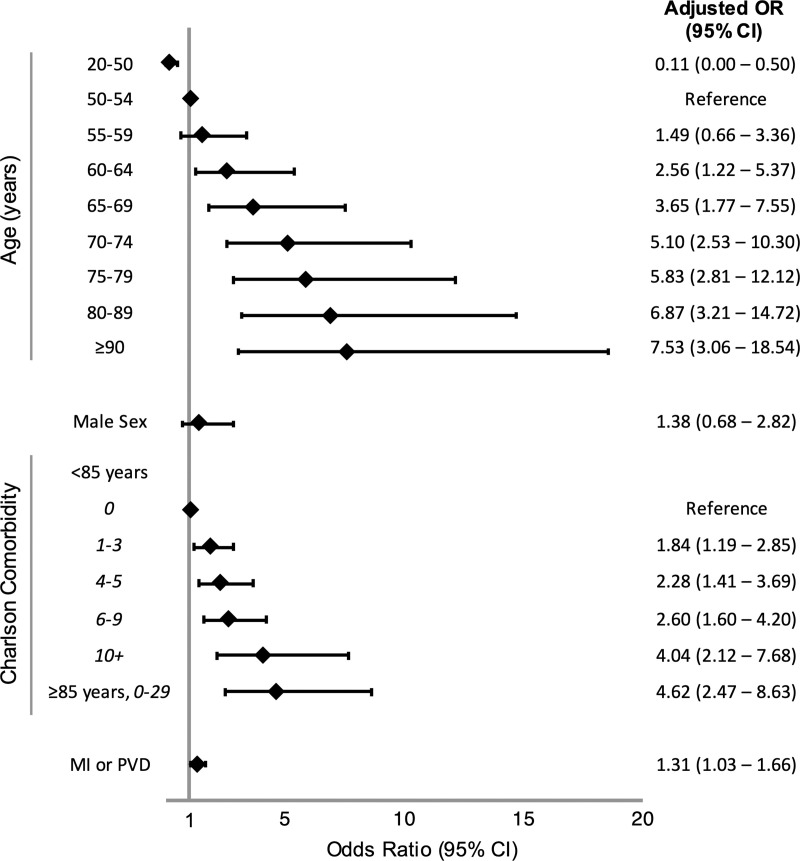
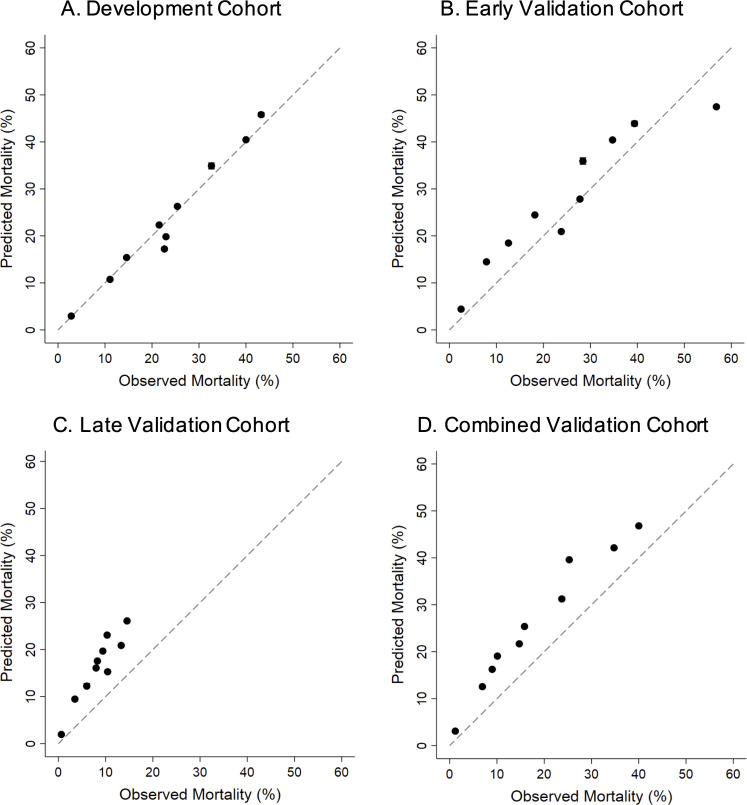
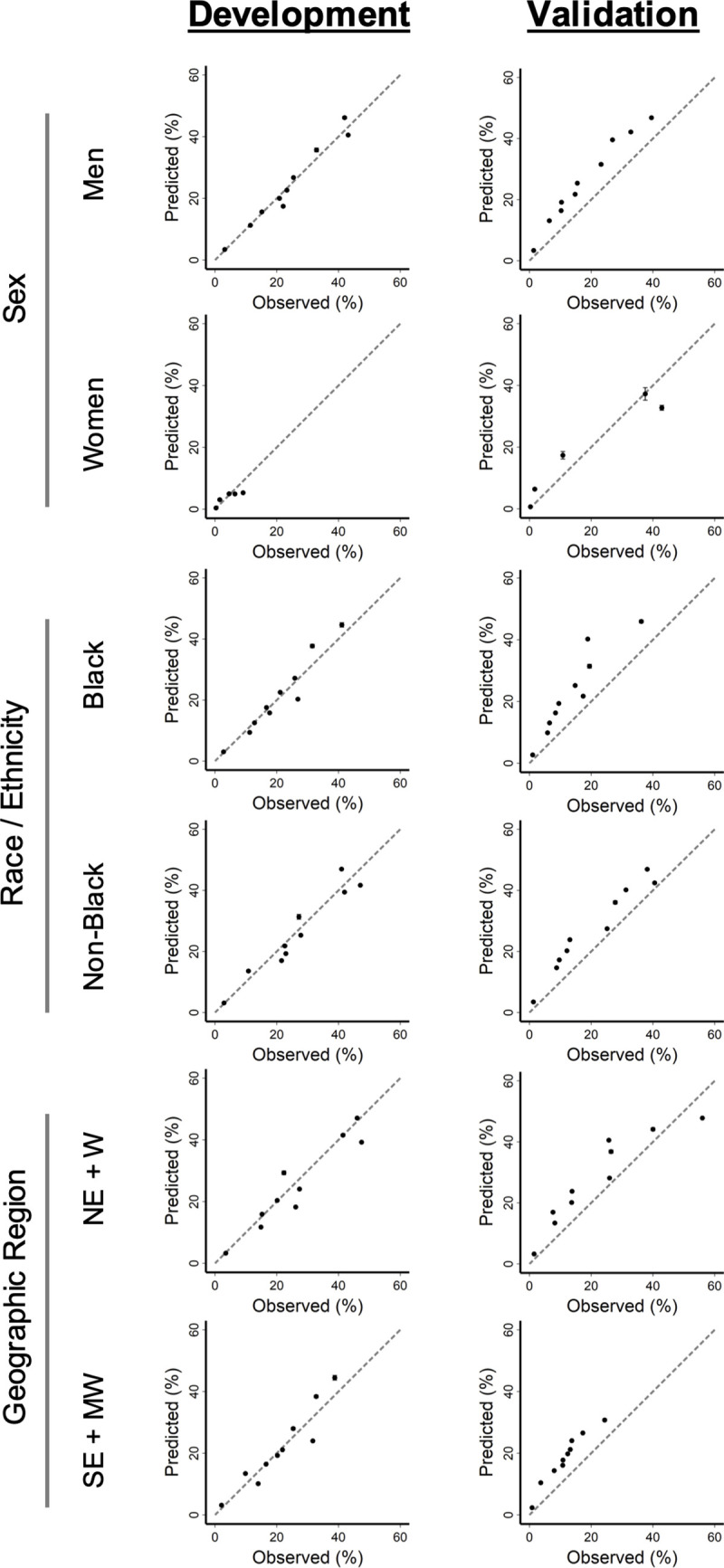
We reviewed SARS-CoV-2 testing results within the VA between February 8 and August 18, 2020. The sample was split into a development cohort (test positive between March 2 and April 15, 2020), an early validation cohort (test positive between April 16 and May 18, 2020), and a late validation cohort (test positive between May 19 and July 19, 2020). Our logistic regression model in the development cohort considered demographics (age, sex, race/ethnicity), and pre-existing medical conditions and the Charlson Comorbidity Index (CCI) derived from ICD-10 diagnosis codes. Weights were fixed to create the VACO Index that was then validated by comparing area under receiver operating characteristic curves (AUC) in the early and late validation cohorts and among important validation cohort subgroups defined by sex, race/ethnicity, and geographic region. We also evaluated calibration curves and the range of predictions generated within age categories. 13,323 individuals tested positive for SARS-CoV-2 (median age: 63 years; 91% male; 42% non-Hispanic Black). We observed 480/3,681 (13%) deaths in development, 253/2,151 (12%) deaths in the early validation cohort, and 403/7,491 (5%) deaths in the late validation cohort. Age, multimorbidity described with CCI, and a history of myocardial infarction or peripheral vascular disease were independently associated with mortality-no other individual comorbid diagnosis provided additional information. The VACO Index discriminated mortality in development (AUC = 0.79, 95% CI: 0.77-0.81), and in early (AUC = 0.81 95% CI: 0.78-0.83) and late (AUC = 0.84, 95% CI: 0.78-0.86) validation. The VACO Index allows personalized estimates of 30-day mortality after COVID-19 infection. For example, among those aged 60-64 years, overall mortality was estimated at 9% (95% CI: 6-11%). The Index further discriminated risk in this age stratum from 4% (95% CI: 3-7%) to 21% (95% CI: 12-31%), depending on sex and comorbid disease.
Prior to infection, demographics and comorbid conditions can discriminate COVID-19 mortality risk overall and within age strata. The VACO Index reproducibly identified individuals at substantial risk of COVID-19 mortality who might consider continuing social distancing, despite relaxed state and local guidelines.
现有的 COVID-19 死亡率指数仅限于急性住院数据。我们利用美国退伍军人事务部(VA)在 SARS-CoV-2 感染之前提供的全国性医疗管理数据,开发了 VA COVID-19(VACO)30 天死亡率指数,并在两个独立的前瞻性样本中验证了该指数。
我们回顾了 2020 年 2 月 8 日至 8 月 18 日期间 VA 内的 SARS-CoV-2 检测结果。该样本分为开发队列(2020 年 3 月 2 日至 4 月 15 日期间检测呈阳性)、早期验证队列(2020 年 4 月 16 日至 5 月 18 日期间检测呈阳性)和晚期验证队列(2020 年 5 月 19 日至 7 月 19 日期间检测呈阳性)。我们的开发队列中的逻辑回归模型考虑了人口统计学特征(年龄、性别、种族/民族)、以及预先存在的医疗条件和 Charlson 合并症指数(CCI),该指数源自 ICD-10 诊断代码。我们固定权重以创建 VACO 指数,然后通过比较早期和晚期验证队列中的接收者操作特征曲线(AUC)、根据性别、种族/民族和地理区域定义的重要验证队列亚组中的 AUC 来验证该指数。我们还评估了校准曲线和年龄类别内的预测范围。共有 13323 人 SARS-CoV-2 检测呈阳性(中位数年龄:63 岁;91%为男性;42%为非西班牙裔黑人)。我们在开发队列中观察到 480/3681(13%)例死亡,在早期验证队列中观察到 253/2151(12%)例死亡,在晚期验证队列中观察到 403/7491(5%)例死亡。年龄、CCI 描述的多态性以及心肌梗死或外周血管疾病史与死亡率独立相关——没有其他单独的合并症诊断提供了额外的信息。VACO 指数在开发队列中区分了死亡率(AUC = 0.79,95%CI:0.77-0.81),在早期(AUC = 0.81,95%CI:0.78-0.83)和晚期(AUC = 0.84,95%CI:0.78-0.86)验证队列中也区分了死亡率。VACO 指数可以在 COVID-19 感染后个性化估计 30 天死亡率。例如,在 60-64 岁年龄组中,总体死亡率估计为 9%(95%CI:6-11%)。该指数进一步区分了这一年龄组内取决于性别和合并症的风险,从 4%(95%CI:3-7%)到 21%(95%CI:12-31%)。
在感染之前,人口统计学特征和合并症可以总体上和在年龄分层中区分 COVID-19 死亡率风险。VACO 指数可重现性地识别出具有 COVID-19 死亡高风险的个体,尽管州和地方的指导方针已经放宽,但这些个体可能仍会考虑继续保持社交距离。