Department of Radiology, University College London Hospital NHS Foundation Trust, London, UK.
Division of Surgery & Interventional Science, University College London, 3rd Floor, Charles Bell House, 43-45 Foley St., London, W1W 7TS, UK.
Eur Radiol. 2021 Mar;31(3):1644-1655. doi: 10.1007/s00330-020-07256-z. Epub 2020 Sep 30.
The PRECISE recommendations for magnetic resonance imaging (MRI) in patients on active surveillance (AS) for prostate cancer (PCa) include repeated measurement of each lesion, and attribution of a PRECISE radiological progression score for the likelihood of clinically significant change over time. We aimed to compare the PRECISE score with clinical progression in patients who are managed using an MRI-led AS protocol.
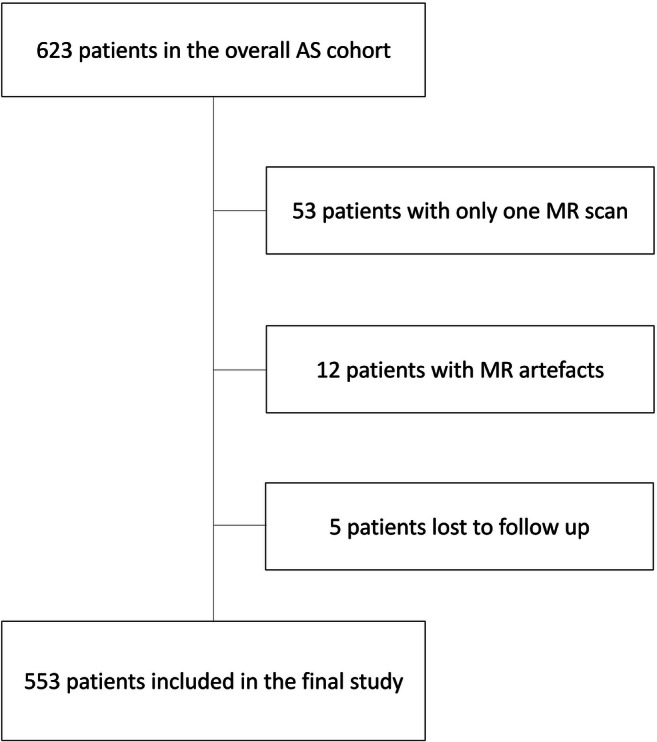
A total of 553 patients on AS for low- and intermediate-risk PCa (up to Gleason score 3 + 4) who had two or more MRI scans performed between December 2005 and January 2020 were included. Overall, 2161 scans were retrospectively re-reported by a dedicated radiologist to give a PI-RADS v2 score for each scan and assess the PRECISE score for each follow-up scan. Clinical progression was defined by histological progression to ≥ Gleason score 4 + 3 (Gleason Grade Group 3) and/or initiation of active treatment. Progression-free survival was assessed using Kaplan-Meier curves and log-rank test was used to assess differences between curves.
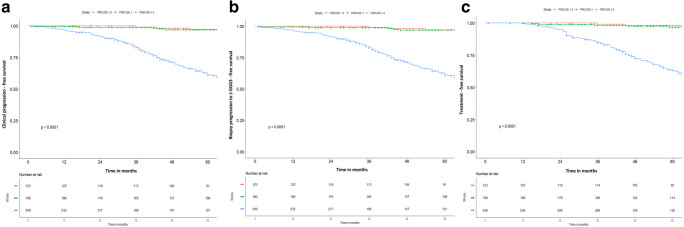
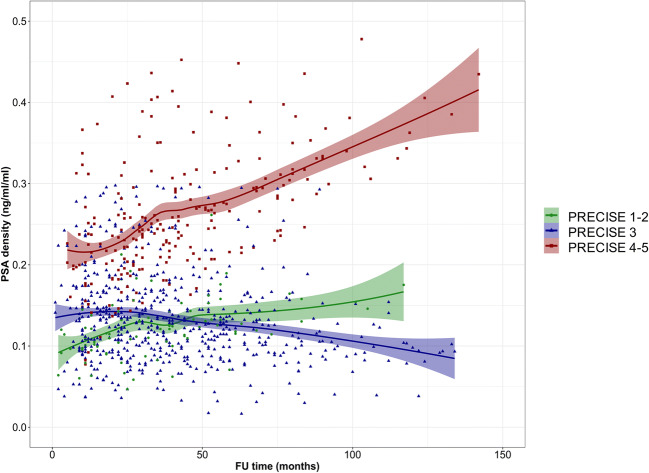
Overall, 165/553 (30%) patients experienced the primary outcome of clinical progression (median follow-up, 74.5 months; interquartile ranges, 53-98). Of all patients, 313/553 (57%) did not show radiological progression on MRI (PRECISE 1-3), of which 296/313 (95%) had also no clinical progression. Of the remaining 240/553 patients (43%) with radiological progression on MRI (PRECISE 4-5), 146/240 (61%) experienced clinical progression (p < 0.0001). Patients with radiological progression on MRI (PRECISE 4-5) showed a trend to an increase in PSA density.
Patients without radiological progression on MRI (PRECISE 1-3) during AS had a very low likelihood of clinical progression and many could avoid routine re-biopsy.
• Patients without radiological progression on MRI (PRECISE 1-3) during AS had a very low likelihood of clinical progression and many could avoid routine re-biopsy. • Clinical progression was almost always detectable in patients with radiological progression on MRI (PRECISE 4-5) during AS. • Patients with radiological progression on MRI (PRECISE 4-5) during AS showed a trend to an increase in PSA density.
针对接受主动监测(AS)的前列腺癌(PCa)患者,磁共振成像(MRI)的 PRECISE 建议包括对每个病灶进行重复测量,并对每个病灶的 PRECISE 影像学进展评分进行赋值,以评估随时间推移发生临床显著变化的可能性。我们旨在比较采用 MRI 引导的 AS 方案治疗的患者中 PRECISE 评分与临床进展的关系。
共纳入 553 例接受低危和中危 PCa(最高 Gleason 评分 3+4)AS 的患者,他们在 2005 年 12 月至 2020 年 1 月期间进行了两次或两次以上的 MRI 检查。共有 2161 次扫描由一名专门的放射科医生进行回顾性重新报告,以获得每个扫描的 PI-RADS v2 评分,并评估每个随访扫描的 PRECISE 评分。临床进展定义为组织学进展至≥Gleason 评分 4+3(Gleason 分级组 3)和/或开始积极治疗。使用 Kaplan-Meier 曲线评估无进展生存率,并使用对数秩检验比较曲线之间的差异。
总体而言,553 例患者中有 165 例(30%)发生了临床进展的主要结局(中位随访时间为 74.5 个月;四分位距为 53-98)。在所有患者中,313 例(57%)MRI 未见影像学进展(PRECISE 1-3),其中 296 例(95%)也无临床进展。在其余 240 例(43%)MRI 显示影像学进展(PRECISE 4-5)的患者中,146 例(61%)发生了临床进展(p<0.0001)。MRI 显示影像学进展(PRECISE 4-5)的患者,PSA 密度呈上升趋势。
AS 期间 MRI 未见影像学进展(PRECISE 1-3)的患者发生临床进展的可能性非常低,许多患者可避免常规再次活检。
AS 期间 MRI 未见影像学进展(PRECISE 1-3)的患者发生临床进展的可能性非常低,许多患者可避免常规再次活检。
AS 期间 MRI 显示影像学进展(PRECISE 4-5)的患者,临床进展几乎总是可检测到。
AS 期间 MRI 显示影像学进展(PRECISE 4-5)的患者 PSA 密度呈上升趋势。