Regnery Sebastian, Behl Nicolas G R, Platt Tanja, Weinfurtner Nina, Windisch Paul, Deike-Hofmann Katerina, Sahm Felix, Bendszus Martin, Debus Jürgen, Ladd Mark E, Schlemmer Heinz-Peter, Rieken Stefan, Adeberg Sebastian, Paech Daniel
Department of Radiation Oncology, Heidelberg University Hospital, Im Neuenheimer Feld 400, 69120 Heidelberg, Germany; Clinical Cooperation Unit Radiation Oncology, German Cancer Research Center (DKFZ), Im Neuenheimer Feld 280, 69120 Heidelberg, Germany.
Siemens Healthcare GmbH, Erlangen, Germany; Division of Medical Physics in Radiology, German Cancer Research Center (DKFZ), Im Neuenheimer Feld 280, 69120 Heidelberg, Germany.
Neuroimage Clin. 2020;28:102427. doi: 10.1016/j.nicl.2020.102427. Epub 2020 Sep 12.
This prospective clinical trial investigated sodium (Na) MRI at 7 Tesla (T) field strength as biomarker for tumor extent, isocitrate dehydrogenase (IDH) mutation and O6-methylguanine DNA methyltransferase (MGMT) promotor methylation in glioma patients.
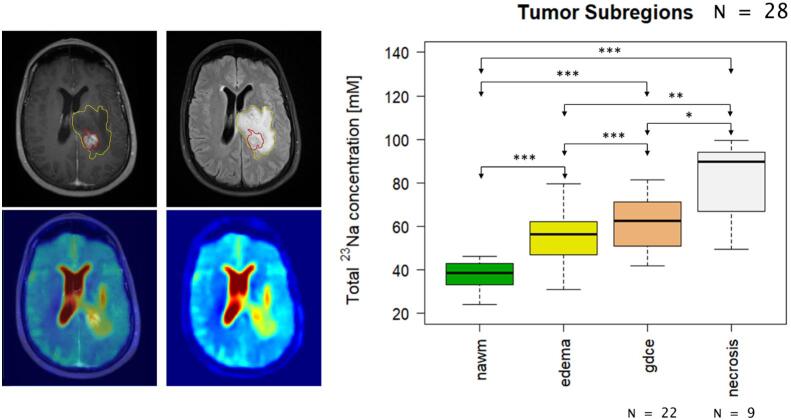
28 glioma patients underwent Na MRI on a 7T scanner (Siemens Healthcare, Erlangen, Germany) parallel to standard 3T MRI before chemoradiation. Areas of Gadolinium-contrast enhancement (gdce), non-enhancing T2-hyperintensity (regarded as edema), necrosis, and normal-appearing white matter (nawm) were segmented on 3T MRI imaging and were co-registered with the Na images. The median total Na concentrations of all areas were compared by pairwise t-tests. Furthermore, areas of gdce and edema were merged to yield the whole tumor area without necrosis. Subsequently, the difference in median of the Na concentration of this whole tumor area was compared between IDH-mutated and IDH wild-type gliomas as well as MGMT methylated and MGMT not-methylated glioblastomas using Whitney-Mann U-tests. All p-values were corrected after the Bonferroni-Holm procedure.
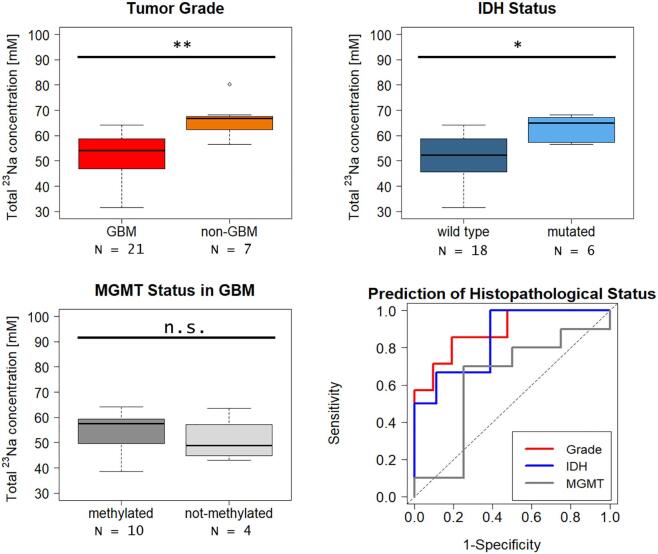
The Na concentration increased successively from nawm to necrotic areas (mean ± sd: nawm = 37.84 ± 5.87 mM, edema = 54.69 ± 10.64 mM, gdce = 61.72 ± 12.95 mM, necrosis = 81.88 ± 17.53 mM) and the concentrations differed statistically significantly between all regarded areas (adjusted p-values for all pairwise comparisons < 0.05). Furthermore, IDH-mutated gliomas showed significantly higher Na concentrations than IDH wild-type gliomas (median [interquartile range]: IDH wild-type = 52.37 mM [45.98 - 58.56 mM], IDH mutated = 65.02 mM [58.87-67.05 mM], p = 0.039). Among the glioblastomas, there was a trend towards increased Na concentration in MGMT methylated tumors that did not reach statistical significance (median [interquartile range]: MGMT methylated = 57.59 mM [50.70 - 59.17 mM], MGMT not methylated = 48.78 mM [45.88 - 53.91 mM], p = 1.0).
Na MRI correlates with the IDH mutation status and could therefore enhance image guidance towards biopsy sites as wells as image-guided surgery and radiotherapy. Furthermore, the successive decrease of Na concentration from central necrosis to normal-appearing white matter suggests a correlation with tumor infiltration.
本前瞻性临床试验研究了7特斯拉(T)场强下的钠(Na)磁共振成像(MRI)作为胶质瘤患者肿瘤范围、异柠檬酸脱氢酶(IDH)突变和O6-甲基鸟嘌呤-DNA甲基转移酶(MGMT)启动子甲基化生物标志物的情况。
28例胶质瘤患者在放化疗前,于7T扫描仪(西门子医疗,德国埃尔朗根)上进行Na MRI检查,同时并行标准3T MRI检查。在3T MRI图像上对钆对比增强(gdce)区域、非增强T2高信号(视为水肿)区域、坏死区域及正常外观白质(nawm)进行分割,并与Na图像进行配准。通过两两t检验比较所有区域的钠总浓度中位数。此外,将gdce区域和水肿区域合并以获得无坏死的整个肿瘤区域。随后,使用惠特尼-曼恩U检验比较IDH突变型和IDH野生型胶质瘤以及MGMT甲基化和MGMT未甲基化胶质母细胞瘤之间该整个肿瘤区域钠浓度中位数的差异。所有p值在进行邦费罗尼-霍尔姆校正后得出。
钠浓度从nawm到坏死区域依次升高(均值±标准差:nawm = 37.84±5.87 mM,水肿 = 54.69±10.64 mM,gdce = 61.72±12.95 mM,坏死 = 81.88±17.53 mM),且所有相关区域之间的浓度差异具有统计学意义(所有两两比较的校正p值<0.05)。此外,IDH突变型胶质瘤的钠浓度显著高于IDH野生型胶质瘤(中位数[四分位间距]:IDH野生型 = 52.37 mM [45.98 - 58.56 mM],IDH突变型 = 65.02 mM [58.87 - 67.05 mM],p = 0.039)。在胶质母细胞瘤中,MGMT甲基化肿瘤的钠浓度有升高趋势,但未达到统计学意义(中位数[四分位间距]:MGMT甲基化 = 57.59 mM [50.70 - 59.17 mM],MGMT未甲基化 = 48.78 mM [45.88 - 53.91 mM],p = 1.0)。
Na MRI与IDH突变状态相关,因此可增强对活检部位的图像引导以及图像引导手术和放疗。此外,从中央坏死到正常外观白质钠浓度的逐渐降低提示与肿瘤浸润相关。