Anesthesiology, New York-Presbyterian Hospital/Weill Cornell Medical Center, New York, New York, USA
Anesthesiology, New York-Presbyterian Hospital/Weill Cornell Medical Center, New York, New York, USA.
Reg Anesth Pain Med. 2020 Dec;45(12):979-984. doi: 10.1136/rapm-2020-101728. Epub 2020 Oct 1.
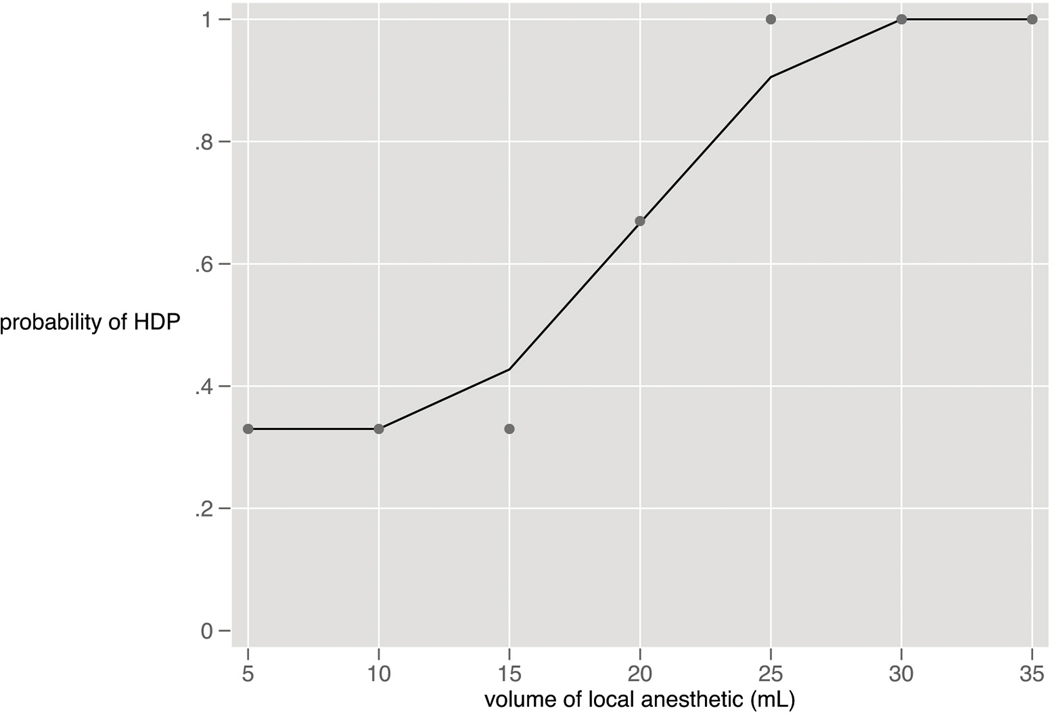
There is no consensus regarding what volume of local anesthetic should be used to achieve successful supraclavicular block while minimizing hemidiaphragmatic paresis (HDP). This study investigated the dose-response relationship between local anesthetic volume and HDP after ultrasound-guided supraclavicular brachial plexus block.
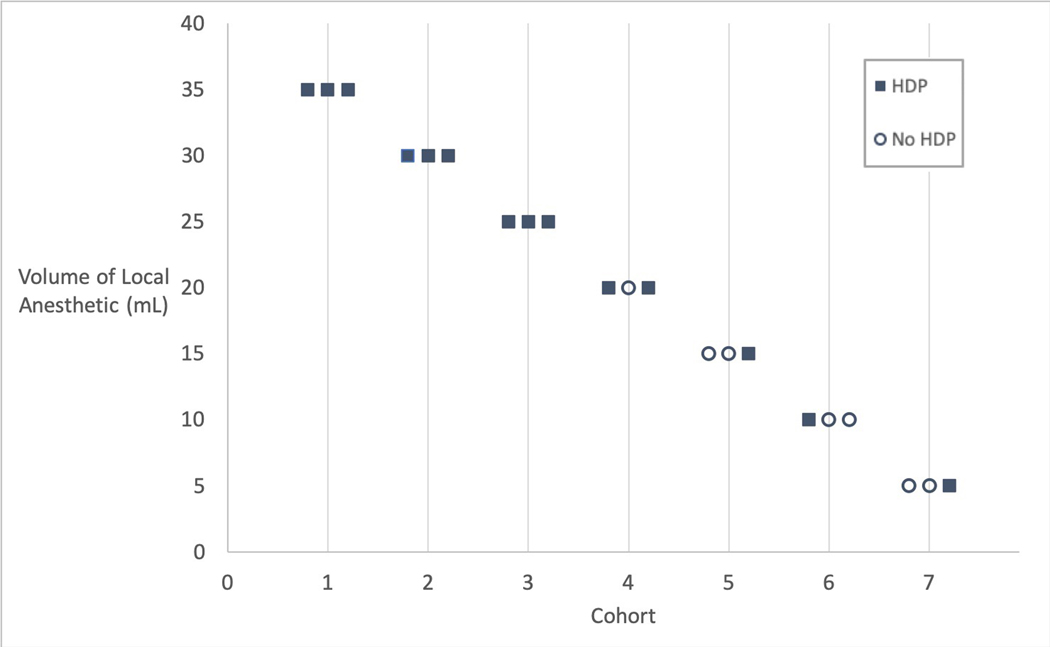
A dose escalation design was used to define the dose response curve for local anesthetic volume and incidence of HDP in subjects undergoing upper extremity surgery with supraclavicular block as the primary anesthetic. Dosing levels of 5, 10, 15, 20, 25, 30, 35 and 40 mL of local anesthetic were administered in cohorts of three subjects per dose. Diaphragm function was assessed with M-mode ultrasound before and after block. Secondary objectives included assessment of negative inspiratory force (NIF), oxygen saturation, subjective dyspnea and extent of sensory and motor blockade.
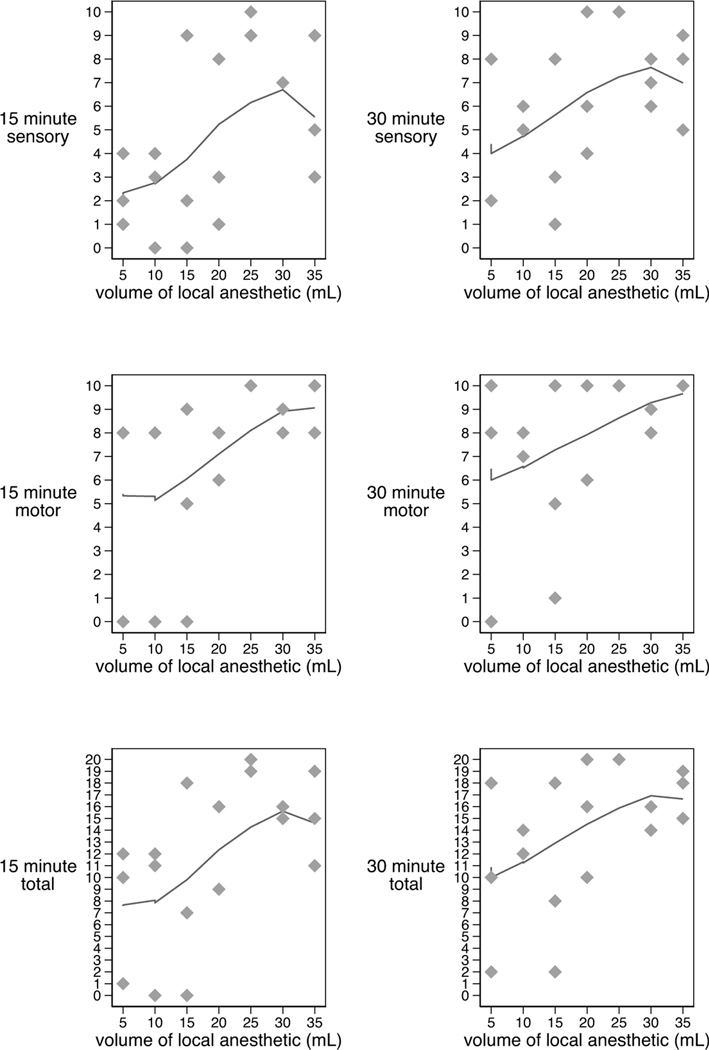
Twenty-one subjects completed the study. HDP was present at all doses, with an incidence of 33% at 5 mL to 100% at 30-35 mL. There was a significant decrease in NIF (7.5 cmHO, IQR (22,0); p=0.01) and oxygen saturation on room air (1%, IQR (2,0); p=0.01) 30 min postblock in subjects experiencing HDP but not in those without HDP. There was no increase in dyspnea in subjects with or without HDP. No subject required respiratory intervention. Motor and sensory block improved with increasing dose, and subjects with HDP exhibited denser blocks than those without (p<0.01).
There is no clinically relevant volume of local anesthetic at which HDP can be avoided when performing a supraclavicular block. In our subject population free of respiratory disease, HDP was well tolerated.
NCT03138577.
在超声引导锁骨上臂丛阻滞中,为了实现成功的锁骨上阻滞并最小化膈肌麻痹(HDP),尚不存在关于应使用多少局部麻醉药容量的共识。本研究旨在调查局部麻醉药容量与 HDP 之间的剂量反应关系,该研究纳入了接受锁骨上阻滞的上肢手术患者。
采用剂量递增设计来定义局部麻醉药容量和 HDP 发生率的剂量反应曲线,锁骨上阻滞为主要麻醉方法。5、10、15、20、25、30、35 和 40 mL 剂量水平的局部麻醉药以每剂量 3 名受试者的队列给予。在阻滞前后使用 M 模式超声评估膈肌功能。次要目标包括评估负吸气力(NIF)、氧饱和度、主观呼吸困难以及感觉和运动阻滞的程度。
21 名受试者完成了研究。所有剂量均出现 HDP,5 mL 时有 33%的发生率,30-35 mL 时有 100%的发生率。在发生 HDP 的受试者中,NIF 显著降低(7.5 cmHO,IQR(22,0);p=0.01),在阻塞后 30 分钟,在空气中的氧饱和度降低(1%,IQR(2,0);p=0.01),而在无 HDP 的受试者中没有观察到这种变化。在有或没有 HDP 的受试者中,呼吸困难均无增加。没有受试者需要呼吸干预。随着剂量的增加,运动和感觉阻滞得到改善,且有 HDP 的受试者的阻滞程度比无 HDP 的更密集(p<0.01)。
在进行锁骨上阻滞时,无法避免 HDP 的发生,因为局部麻醉药的容量没有临床相关性。在我们的无呼吸系统疾病的受试者人群中,HDP 是可以耐受的。
NCT03138577。