Hu Zhenfa, Hu Jinge, Ai Zhangran, Xu Songchao, Li Huili, Guo Ruijuan, Wang Yun
Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People's Republic of China.
J Pain Res. 2024 Dec 20;17:4453-4462. doi: 10.2147/JPR.S487562. eCollection 2024.
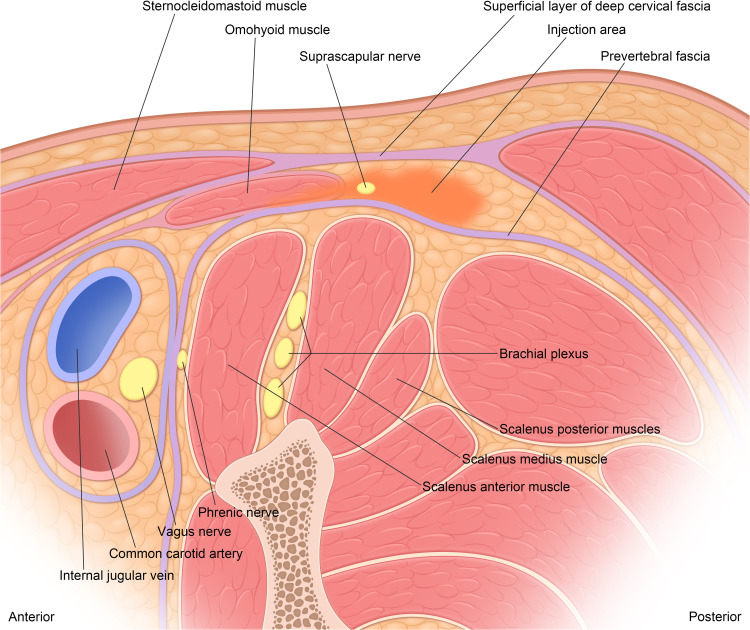
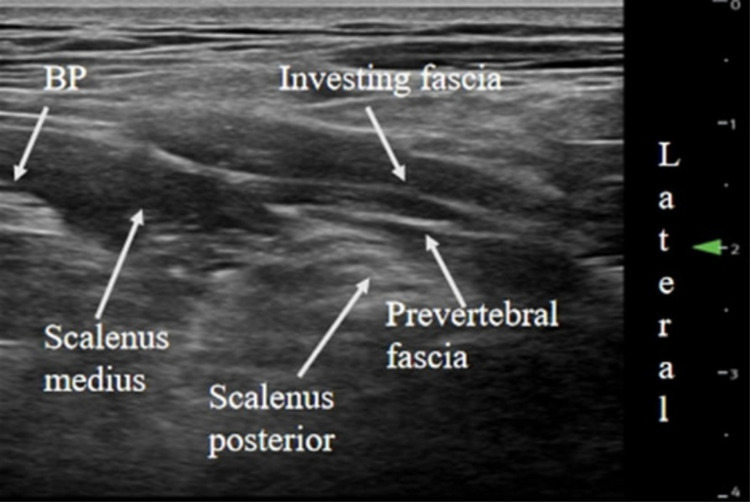
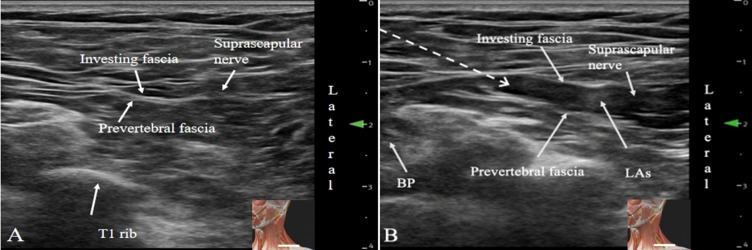
The suprascapular nerve is situated between the prevertebral fascia and the superficial layer of deep cervical fascia and on the surface of the middle and posterior scalene muscles before it reaches the suprascapular notch. Consequently, we hypothesized that injecting local anesthetics (LAs) there would introduce a new block approach for blocking the suprascapular nerve, ie, extra-prevertebral fascial block. We assessed the postoperative analgesic effect, as well as the incidence of diaphragmatic paralysis 30 minutes after the block.
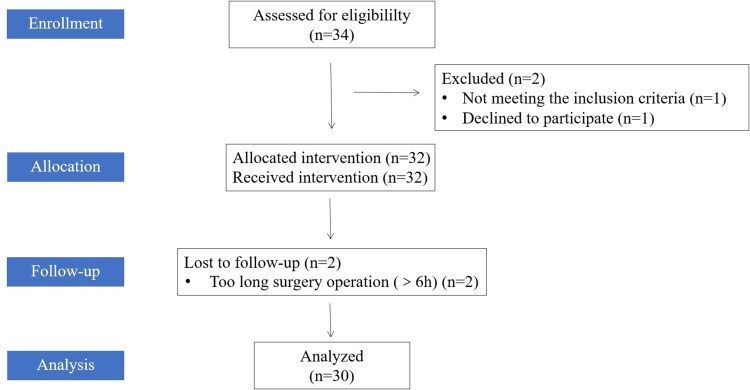
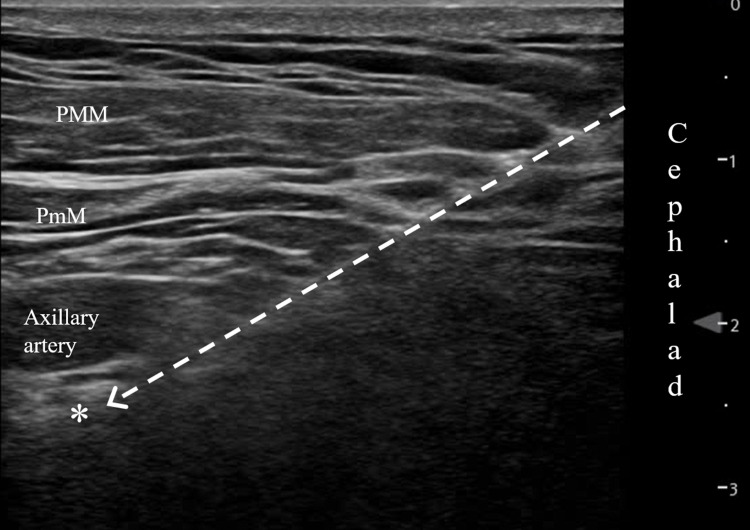
30 patients undergoing elective shoulder arthroscopic rotator cuff repair surgery were recruited in this study. Before the induction of general anesthesia, 15 mL of 0.5% ropivacaine was administered to perform an extra-prevertebral fascia suprascapular nerve block (10 mL) and an infraclavicular brachial plexus block (5 mL, primarily targeting the axillary nerve). All patients received intravenous patient-controlled analgesia (PCA) after surgery. The postoperative pain was scored with Numeric Rating Scale (NRS), along with the opioid consumption in the first 24 h after surgery. The incidence of hemi-diaphragmatic paralysis (HDP) was measured 30 minutes after the block.
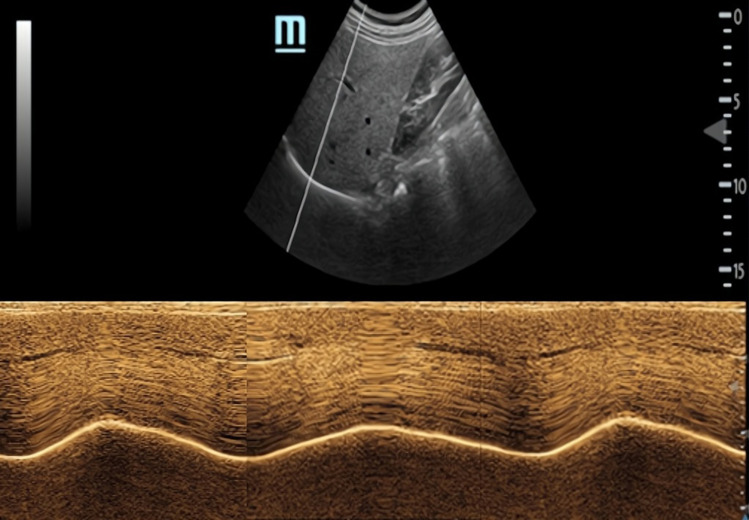
All patients received the successful block. The resting NRS pain scores at 1h, 6h, 12h, and 24h postoperatively were 0 [0, 2], 0 [0, 2], 1 [0, 2], and 2 [1, 3], respectively. The oral morphine equivalent (OME) consumption at 24 hours after surgery was 18 [12,30] mg. No patients experienced HDP (complete or partial) 30 minutes after the block.
Compared with the posterior approach, this novel technique is efficient and has a higher success rate of blockade. It eliminates the need for patients to change positions, thereby improving comfort. Additionally, when combined with the infraclavicular brachial plexus block, it can effectively block the suprascapular nerve, providing satisfactory postoperative analgesia without the HDP at 30min after blockade compared to the anterior approach.
肩胛上神经在到达肩胛上切迹之前,位于椎前筋膜和颈深筋膜浅层之间,以及中斜角肌和后斜角肌表面。因此,我们推测在此处注射局部麻醉药(LA)将引入一种新的肩胛上神经阻滞方法,即椎前筋膜外阻滞。我们评估了术后镇痛效果以及阻滞后30分钟膈肌麻痹的发生率。
本研究招募了30例行择期肩关节镜下肩袖修复手术的患者。在全身麻醉诱导前,给予15 mL 0.5%罗哌卡因进行椎前筋膜外肩胛上神经阻滞(10 mL)和锁骨下臂丛神经阻滞(5 mL,主要针对腋神经)。所有患者术后均接受静脉自控镇痛(PCA)。术后疼痛采用数字评分量表(NRS)评分,并记录术后24小时内的阿片类药物消耗量。阻滞后30分钟测量半膈肌麻痹(HDP)的发生率。
所有患者均成功完成阻滞。术后1小时、6小时、12小时和24小时静息状态下的NRS疼痛评分分别为0[0,2]、0[0,2]、1[0,2]和2[1,3]。术后24小时口服吗啡当量(OME)消耗量为18[12,30]mg。阻滞后30分钟,无患者发生HDP(完全或部分)。
与后路阻滞相比,这种新技术有效且阻滞成功率更高。它无需患者改变体位,从而提高了舒适度。此外,与前路阻滞相比,当与锁骨下臂丛神经阻滞联合使用时,它可以有效阻滞肩胛上神经,提供满意的术后镇痛,且阻滞后30分钟不会发生HDP。