Department of Anesthesiology, Pharmacology and Therapeutics, University of British Columbia, Vancouver, British Columbia, Canada.
Center for International Child Health, BC Children's Hospital Research Institute, Vancouver, British Columbia, Canada.
PLoS One. 2020 Oct 2;15(10):e0240092. doi: 10.1371/journal.pone.0240092. eCollection 2020.
Sepsis is the leading cause of death in children under five in low- and middle-income countries. The rapid identification of the sickest children and timely antibiotic administration may improve outcomes. We developed and implemented a digital triage platform to rapidly identify critically ill children to facilitate timely intravenous antibiotic administration.
This quality improvement initiative sought to reduce the time to antibiotic administration at a dedicated children's hospital outpatient department in Mbarara, Uganda.
The digital platform consisted of a mobile application that collects clinical signs, symptoms, and vital signs to prioritize children through a combination of emergency triggers and predictive risk algorithms. A computer-based dashboard enabled the prioritization of children by displaying an overview of all children and their triage categories. We evaluated the impact of the digital triage platform over an 11-week pre-implementation phase and an 11-week post-implementation phase. The time from the end of triage to antibiotic administration was compared to evaluate the quality improvement initiative.
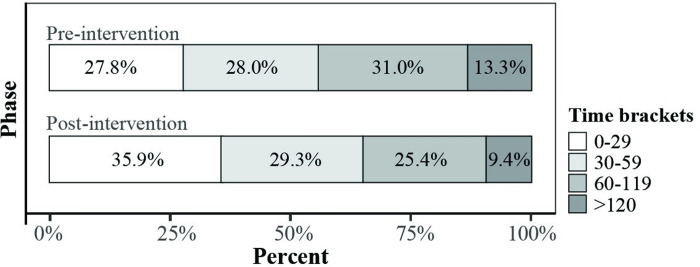
There was a difference of -11 minutes (95% CI, -16.0 to -6.0; p < 0.001; Mann-Whitney U test) in time to antibiotics, from 51 minutes (IQR, 27.0-94.0) pre-implementation to 44 minutes (IQR, 19.0-74.0) post-implementation. Children prioritized as emergency received the greatest time benefit (-34 minutes; 95% CI, -9.0 to -58.0; p < 0.001; Mann-Whitney U test). The proportion of children who waited more than an hour until antibiotics decreased by 21.4% (p = 0.007).
A data-driven patient prioritization and continuous feedback for healthcare workers enabled by a digital triage platform led to expedited antibiotic therapy for critically ill children with sepsis. This platform may have a more significant impact in facilities without existing triage processes and prioritization of treatments, as is commonly encountered in low resource settings.
在中低收入国家,败血症是五岁以下儿童死亡的主要原因。快速识别病情最严重的儿童并及时给予抗生素治疗可能会改善预后。我们开发并实施了一个数字分诊平台,以快速识别危重病儿童,从而及时给予静脉内抗生素治疗。
本质量改进倡议旨在减少乌干达姆巴拉拉市一家儿童医院门诊部给予抗生素的时间。
数字平台由一个移动应用程序组成,该应用程序收集临床体征、症状和生命体征,通过紧急触发和预测风险算法的组合对儿童进行优先排序。一个基于计算机的仪表板通过显示所有儿童及其分诊类别概述来实现儿童的优先排序。我们在实施前的 11 周和实施后的 11 周评估了数字分诊平台的影响。从分诊结束到给予抗生素的时间进行比较,以评估质量改进倡议。
与实施前(51 分钟,IQR,27.0-94.0)相比,时间差异为-11 分钟(95%CI,-16.0 至-6.0;p <0.001;Mann-Whitney U 检验),实施后(44 分钟,IQR,19.0-74.0)抗生素时间更短。被归类为紧急情况的儿童获得的时间收益最大(-34 分钟;95%CI,-9.0 至-58.0;p <0.001;Mann-Whitney U 检验)。等待抗生素治疗超过 1 小时的儿童比例下降了 21.4%(p =0.007)。
通过数字分诊平台实现的数据驱动的患者优先排序和对医护人员的持续反馈,使败血症危重病儿童能够更快地接受抗生素治疗。该平台在没有现有分诊流程和治疗优先级的设施中可能产生更大的影响,这在资源匮乏的环境中很常见。