Isala, Zwolle, The Netherlands.
Department of Epidemiology and Statistics, Isala Academy, Zwolle, The Netherlands.
Int J Infect Dis. 2020 Dec;101:283-289. doi: 10.1016/j.ijid.2020.09.1460. Epub 2020 Sep 29.
The global push for the use of hydroxychloroquine (HCQ) and chloroquine (CQ) against COVID-19 has resulted in an ongoing discussion about the effectivity and toxicity of these drugs. Recent studies report no effect of (H)CQ on 28-day mortality. We investigated the effect of HCQ and CQ in hospitalized patients on the non-ICU COVID-ward.
A nationwide, observational cohort study was performed in The Netherlands. Hospitals were given the opportunity to decide independently on the use of three different COVID-19 treatment strategies: HCQ, CQ, or no treatment. We compared the outcomes between these groups. The primary outcomes were 1) death on the COVID-19 ward, and 2) transfer to the intensive care unit (ICU).
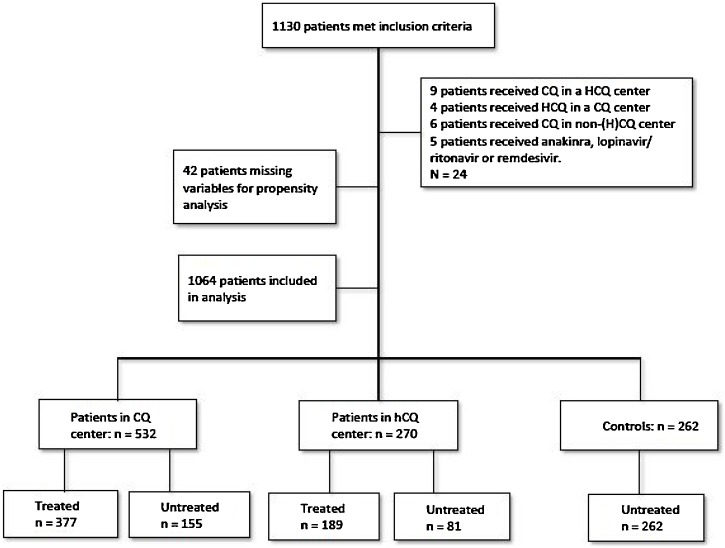
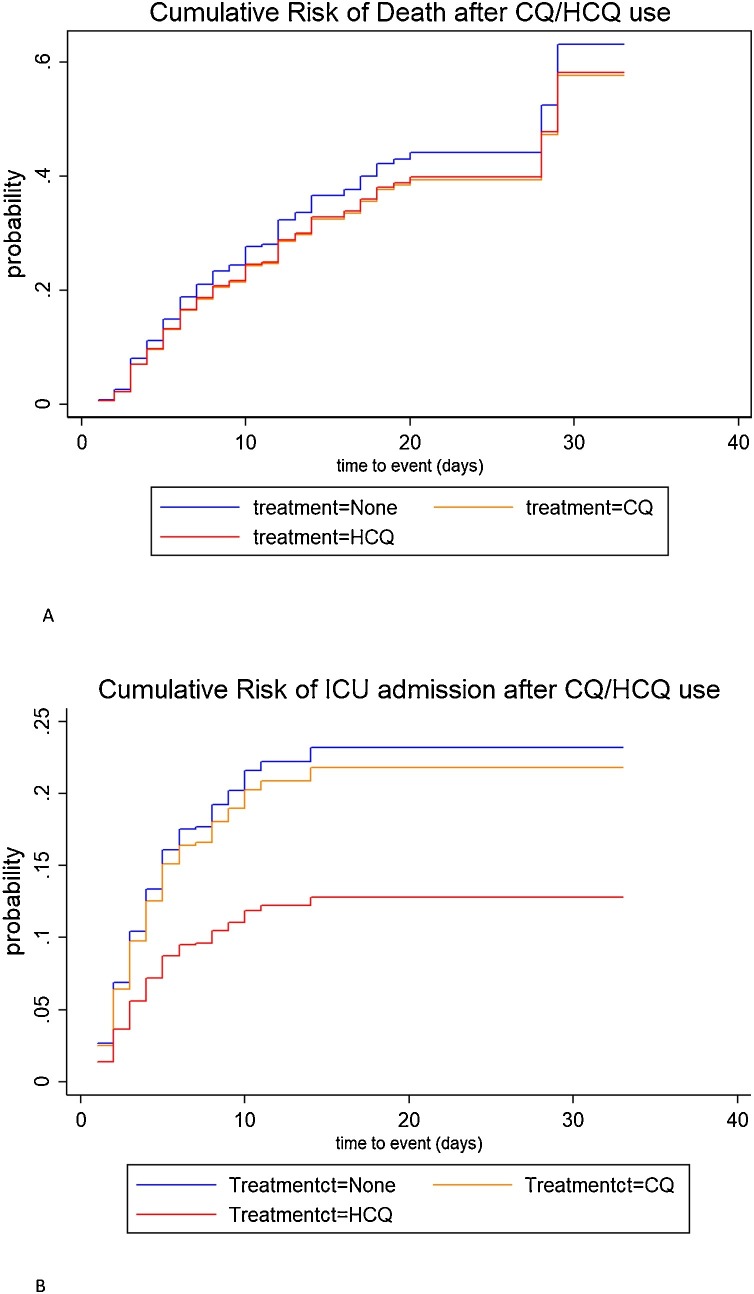
The analysis included 1064 patients from 14 hospitals: 566 patients received treatment with either HCQ (n = 189) or CQ (n = 377), and 498 patients received no treatment. In a multivariate propensity-matched weighted competing regression analysis, there was no significant effect of (H)CQ on mortality on the COVID ward. However, HCQ was associated with a significantly decreased risk of transfer to the ICU (hazard ratio (HR) = 0.47, 95% CI = 0.27-0.82, p = 0.008) when compared with controls. This effect was not found in the CQ group (HR = 0.80, 95% CI = 0.55-1.15, p = 0.207), and remained significant after competing risk analysis.
The results of this observational study demonstrate a lack of effect of (H)CQ on non-ICU mortality. However, we show that the use of HCQ - but not CQ - is associated with a 53% reduction in risk of transfer of COVID-19 patients from the regular ward to the ICU. Recent prospective studies have reported on 28-day, all-cause mortality only; therefore, additional prospective data on the early effects of HCQ in preventing transfer to the ICU are still needed.
全球推动使用羟氯喹(HCQ)和氯喹(CQ)治疗 COVID-19,这导致了对这些药物有效性和毒性的持续讨论。最近的研究报告称,(H)CQ 对 28 天死亡率没有影响。我们调查了住院患者在非 ICU COVID 病房中使用 HCQ 和 CQ 的效果。
在荷兰进行了一项全国性的观察性队列研究。医院有机会独立决定使用三种不同的 COVID-19 治疗策略:HCQ、CQ 或不治疗。我们比较了这些组之间的结果。主要结局是 1)COVID-19 病房死亡,2)转至重症监护病房(ICU)。
该分析包括来自 14 家医院的 1064 名患者:566 名患者接受 HCQ(n=189)或 CQ(n=377)治疗,498 名患者未接受治疗。在多变量倾向评分加权竞争回归分析中,(H)CQ 对 COVID 病房死亡率没有显著影响。然而,与对照组相比,HCQ 显著降低了转 ICU 的风险(危险比(HR)=0.47,95%CI=0.27-0.82,p=0.008)。在 CQ 组中未发现这种作用(HR=0.80,95%CI=0.55-1.15,p=0.207),并且在竞争风险分析后仍然显著。
这项观察性研究的结果表明,(H)CQ 对非 ICU 死亡率没有影响。然而,我们发现使用 HCQ - 而不是 CQ - 与 COVID-19 患者从普通病房转至 ICU 的风险降低 53%相关。最近的前瞻性研究仅报告了 28 天全因死亡率;因此,仍然需要更多关于 HCQ 早期预防转 ICU 的前瞻性数据。