De Giglio Andrea, Mezquita Laura, Auclin Edouard, Blanc-Durand Félix, Riudavets Mariona, Caramella Caroline, Martinez Gala, Benitez Jose Carlos, Martín-Romano Patricia, El-Amarti Lamiae, Hendriks Lizza, Ferrara Roberto, Naltet Charles, Lavaud Pernelle, Gazzah Anas, Adam Julien, Planchard David, Chaput Nathalie, Besse Benjamin
Cancer Medicine Department, Gustave Roussy, 94805 Villejuif, France.
Department of Specialized, Experimental and Diagnostic Medicine, S.Orsola-Malpighi University Hospital, Alma Mater Studiorum University of Bologna, 40126 Bologna, Italy.
Cancers (Basel). 2020 Sep 30;12(10):2827. doi: 10.3390/cancers12102827.
Baseline steroids before ICI have been associated with poor outcomes, particularly when introduced due to cancer symptoms.
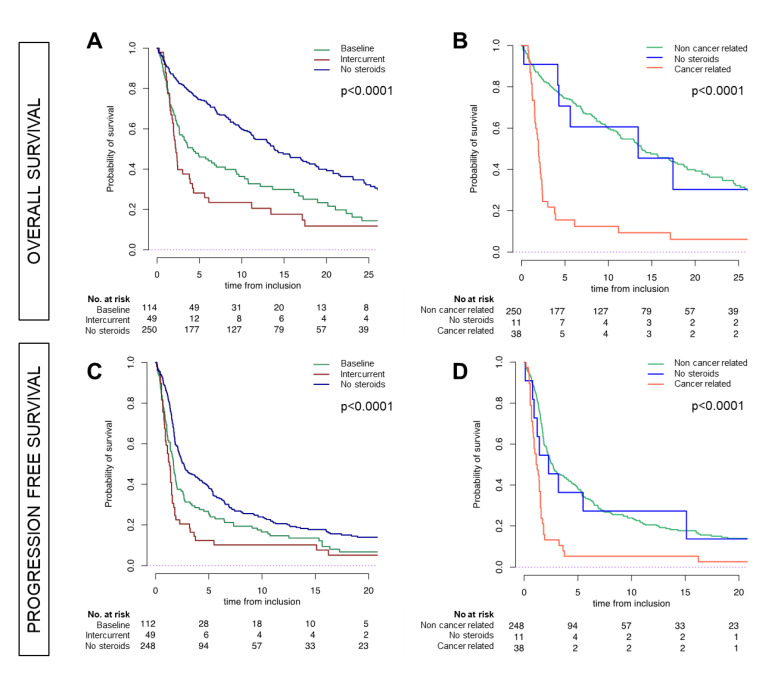
Retrospective analysis of advanced NSCLC patients treated with ICI. We collected the use of intercurrent steroids (≥10 mg of prednisone-equivalent) within the first eight weeks of ICI. We correlated steroid use with patient outcomes according to the indications.
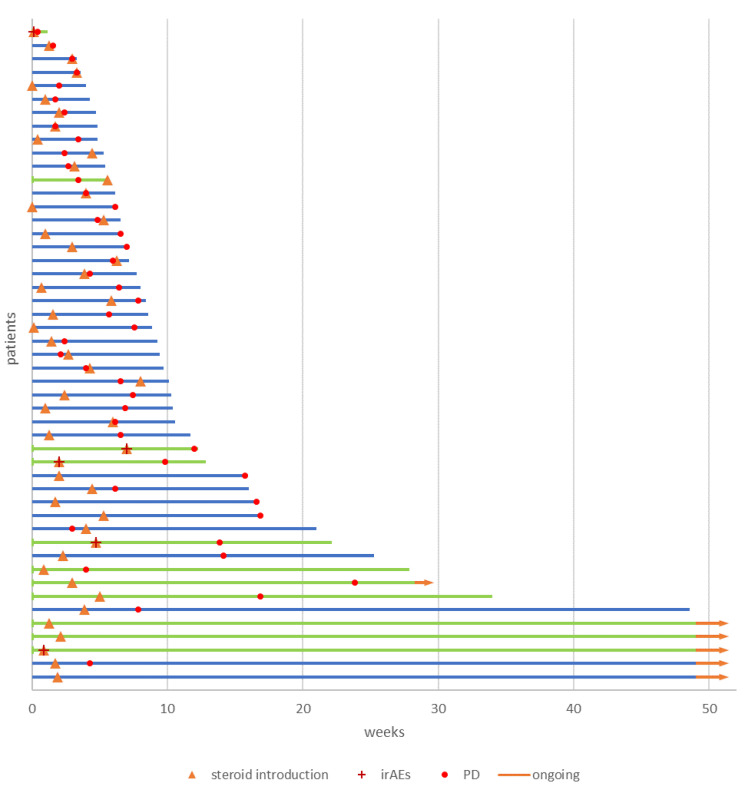
413 patients received ICI, 299 were steroids-naïve at baseline. A total of 49 patients received intercurrent steroids (16%), of whom 38 for cancer-related symptoms and 11 for other indications, such as immune-related events. Overall, median (m) progression-free survival (PFS) was 1.9 months (mo.) [95% CI, 1.8-2.4] and overall survival (OS) 10 mo. [95% CI, 8.1-12.9]. Intercurrent steroids under ICI correlated with a shorter PFS/OS (1.3 and 2.3 mo. respectively, both < 0.0001). Intercurrent steroids for cancer-related symptoms correlated with poorest mPFS [1.1 mo.; 95% CI, 0.9-1.5] and mOS [1.9 mo.; 95%CI, 1.5-2.4; < 0.0001)]. No mOS and mPFS differences were found between cancer-unrelated-steroid group and no-steroid group. Steroid use for cancer-related symptoms was an independent prognostic factor for poor PFS [HR 2.64; 95% CI, 1.2-5.6] and OS [HR 4.53; 95% CI, 1.8-11.1], both < 0.0001.
Intercurrent steroids during ICI had no detrimental prognostic impact if the indication was unrelated to cancer symptoms.
免疫检查点抑制剂(ICI)治疗前使用基线类固醇与不良预后相关,尤其是因癌症症状而使用时。
对接受ICI治疗的晚期非小细胞肺癌(NSCLC)患者进行回顾性分析。我们收集了ICI治疗前八周内使用的并发类固醇(≥10mg泼尼松等效剂量)情况。我们根据用药指征将类固醇使用情况与患者预后进行关联分析。
413例患者接受了ICI治疗,299例在基线时未使用类固醇。共有49例患者使用了并发类固醇(16%),其中38例用于治疗癌症相关症状,11例用于其他指征,如免疫相关事件。总体而言,中位无进展生存期(PFS)为1.9个月(mo.)[95%置信区间(CI),1.8 - 2.4],总生存期(OS)为10个月(mo.)[95%CI,8.1 - 12.9]。ICI治疗期间使用并发类固醇与较短的PFS/OS相关(分别为1.3个月和2.3个月,均P < 0.0001)。用于癌症相关症状的并发类固醇与最差的中位PFS[1.1个月(mo.);95%CI,0.9 - 1.5]和中位OS[1.9个月(mo.);95%CI,1.5 - 2.4;P < 0.0001]相关。在与癌症无关的类固醇使用组和未使用类固醇组之间未发现中位OS和中位PFS差异。用于癌症相关症状的类固醇使用是PFS不良[风险比(HR)2.64;95%CI,1.2 - 5.6]和OS不良[HR 4.53;95%CI,1.8 - 11.1]的独立预后因素,均P < 0.0001。
如果用药指征与癌症症状无关,ICI治疗期间使用并发类固醇对预后无不利影响。