Masson-Grehaigne Cécile, Lafon Mathilde, Palussière Jean, Leroy Laura, Bonhomme Benjamin, Jambon Eva, Italiano Antoine, Cousin Sophie, Crombé Amandine
Department of Diagnostic and Interventional Oncologic Imaging, Institut Bergonié, F-33076 Bordeaux, France.
Department of Radiology, Pellegrin University Hospital, F-33000 Bordeaux, France.
Cancers (Basel). 2024 Jul 8;16(13):2491. doi: 10.3390/cancers16132491.
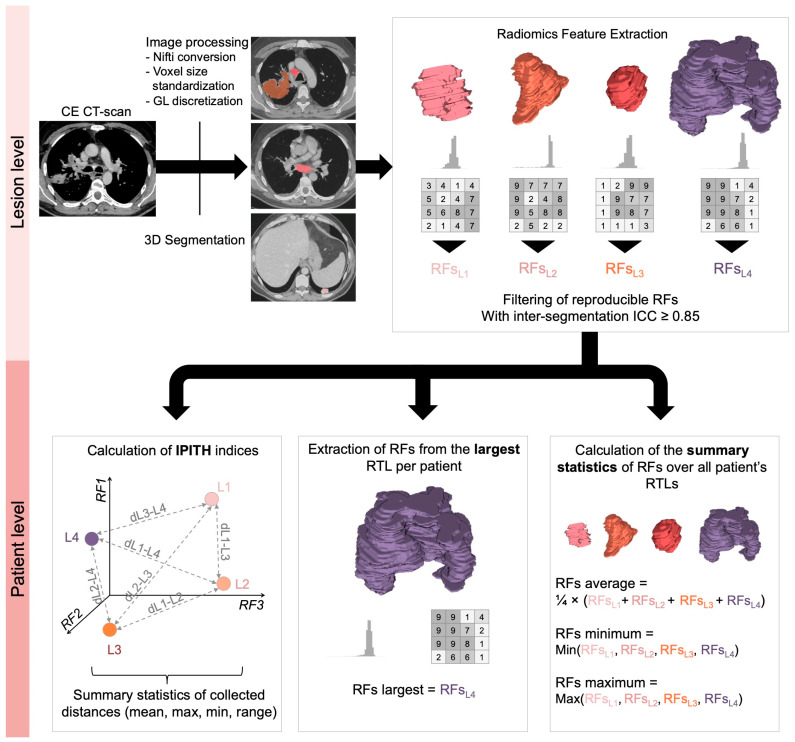
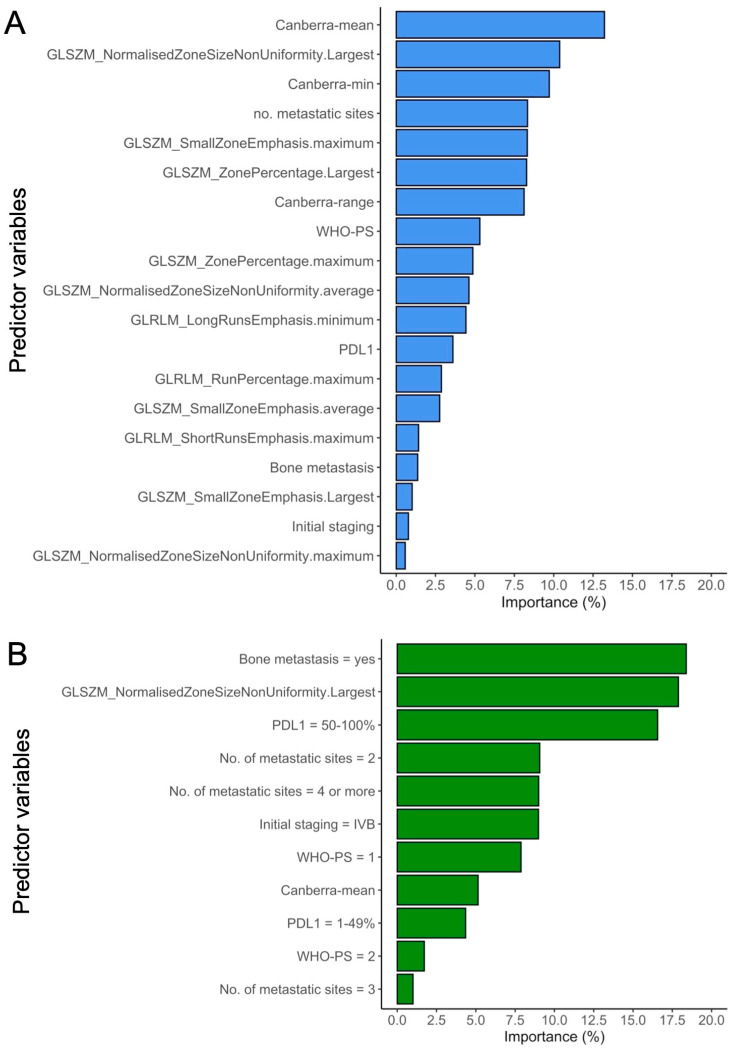
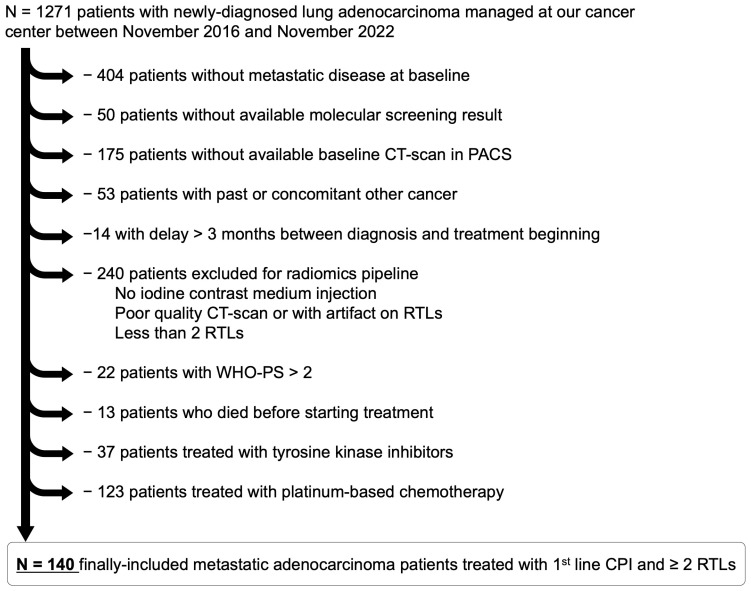
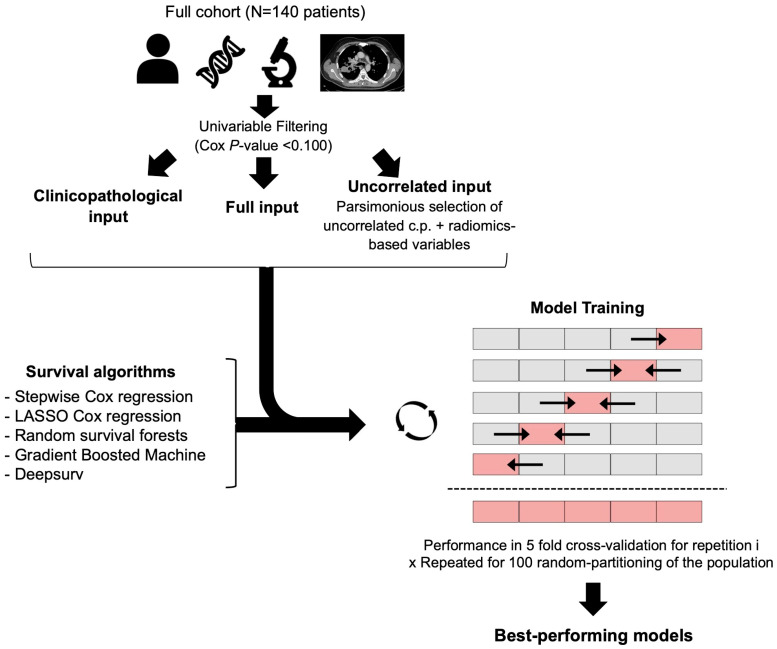
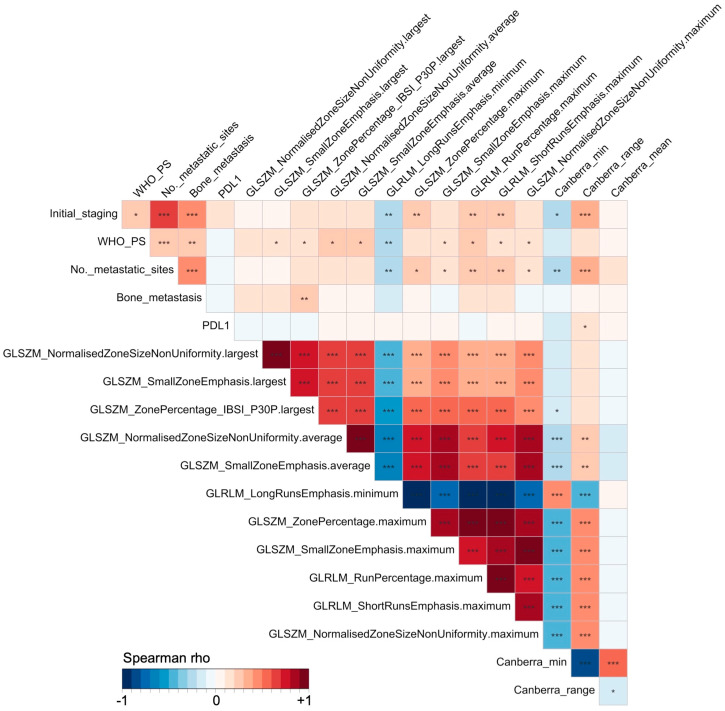
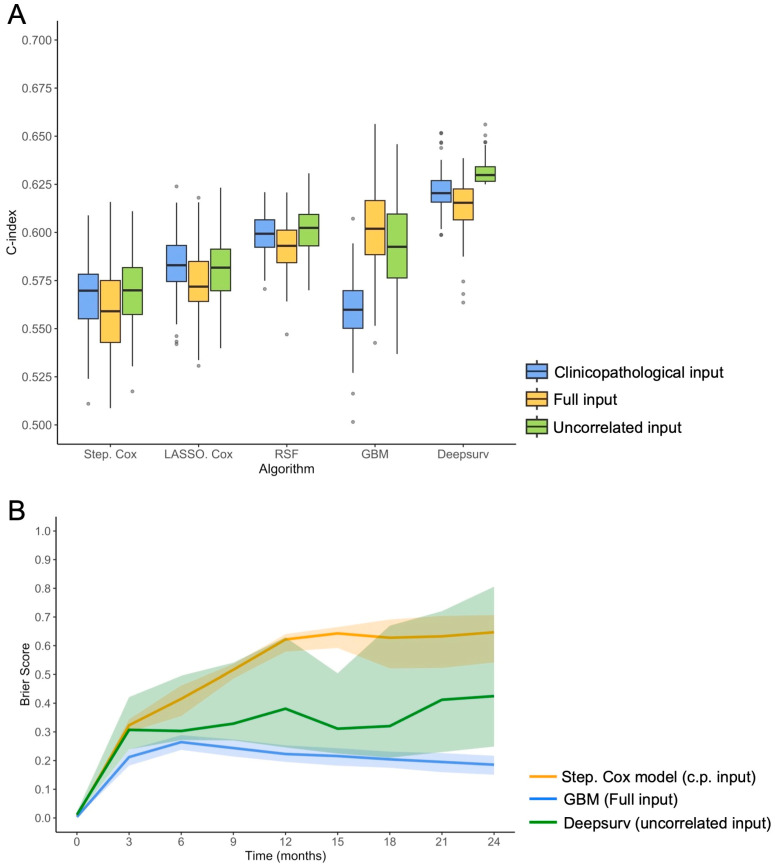
This study aimed to evaluate the potential of pre-treatment CT-based radiomics features (RFs) derived from single and multiple tumor sites, and state-of-the-art machine-learning survival algorithms, in predicting progression-free survival (PFS) for patients with metastatic lung adenocarcinoma (MLUAD) receiving first-line treatment including immune checkpoint inhibitors (CPIs). To do so, all adults with newly diagnosed MLUAD, pre-treatment contrast-enhanced CT scan, and performance status ≤ 2 who were treated at our cancer center with first-line CPI between November 2016 and November 2022 were included. RFs were extracted from all measurable lesions with a volume ≥ 1 cm on the CT scan. To capture intra- and inter-tumor heterogeneity, RFs from the largest tumor of each patient, as well as lowest, highest, and average RF values over all lesions per patient were collected. Intra-patient inter-tumor heterogeneity metrics were calculated to measure the similarity between each patient lesions. After filtering predictors with univariable Cox < 0.100 and analyzing their correlations, five survival machine-learning algorithms (stepwise Cox regression [SCR], LASSO Cox regression, random survival forests, gradient boosted machine [GBM], and deep learning [Deepsurv]) were trained in 100-times repeated 5-fold cross-validation (rCV) to predict PFS on three inputs: (i) clinicopathological variables, (ii) all radiomics-based and clinicopathological (full input), and (iii) uncorrelated radiomics-based and clinicopathological variables (uncorrelated input). The Models' performances were evaluated using the concordance index (c-index). Overall, 140 patients were included (median age: 62.5 years, 36.4% women). In rCV, the highest c-index was reached with Deepsurv (c-index = 0.631, 95%CI = 0.625-0.647), followed by GBM (c-index = 0.603, 95%CI = 0.557-0.646), significantly outperforming standard SCR whatever its input (c-index range: 0.560-0.570, all < 0.0001). Thus, single- and multi-site pre-treatment radiomics data provide valuable prognostic information for predicting PFS in MLUAD patients undergoing first-line CPI treatment when analyzed with advanced machine-learning survival algorithms.
本研究旨在评估源自单个和多个肿瘤部位的基于治疗前CT的放射组学特征(RFs)以及最先进的机器学习生存算法在预测接受包括免疫检查点抑制剂(CPIs)在内的一线治疗的转移性肺腺癌(MLUAD)患者无进展生存期(PFS)方面的潜力。为此,纳入了2016年11月至2022年11月期间在我们癌症中心接受一线CPI治疗的所有新诊断为MLUAD、有治疗前对比增强CT扫描且体能状态≤2的成年人。从CT扫描上所有体积≥1 cm的可测量病变中提取RFs。为了捕捉肿瘤内和肿瘤间的异质性,收集了每位患者最大肿瘤的RFs以及每位患者所有病变的最低、最高和平均RF值。计算患者内肿瘤间异质性指标以测量每位患者病变之间的相似性。在用单变量Cox筛选预测因子<0.100并分析其相关性后,对五种生存机器学习算法(逐步Cox回归[SCR]、LASSO Cox回归、随机生存森林、梯度提升机[GBM]和深度学习[Deepsurv])进行了100次重复的5折交叉验证(rCV)训练,以根据以下三个输入预测PFS:(i)临床病理变量,(ii)所有基于放射组学和临床病理的变量(完整输入),以及(iii)不相关的基于放射组学和临床病理的变量(不相关输入)。使用一致性指数(c指数)评估模型性能。总体而言,纳入了140例患者(中位年龄:62.5岁,女性占36.4%)。在rCV中,Deepsurv达到了最高的c指数(c指数=0.631,95%CI=0.625 - 0.647),其次是GBM(c指数=0.603,95%CI=0.557 - 0.646),无论其输入如何,均显著优于标准SCR(c指数范围:0.560 - 0.570,均<0.0001)。因此,当使用先进的机器学习生存算法进行分析时,单部位和多部位治疗前放射组学数据为预测接受一线CPI治疗的MLUAD患者的PFS提供了有价值的预后信息。