Clinical Epidemiology Team, Paris-Saclay University, Paris-Sud University, UVSQ, CESP, Inserm, Villejuif, France.
Division of Vascular Surgery, Ambroise Paré University Hospital, APHP, Boulogne-Billancourt, France.
BMC Nephrol. 2020 Oct 2;21(1):422. doi: 10.1186/s12882-020-02080-5.
Early kidney transplantation (KT) is the best option for patients with end-stage kidney disease, but little is known about dialysis access strategy in this context. We studied practice patterns of dialysis access and how they relate with outcomes in adults wait-listed early for KT according to the intended donor source.
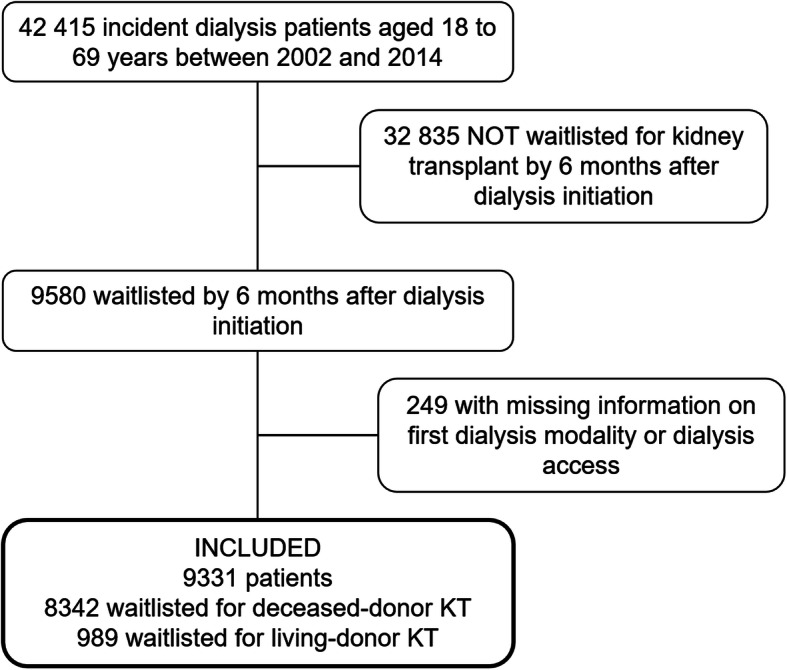
This study from the REIN registry (2002-2014) included 9331 incident dialysis patients (age 18-69) wait-listed for KT before or by 6 months after starting dialysis: 8342 candidates for deceased-donor KT and 989 for living-donor KT. Subdistribution hazard ratios (SHR) of KT and death associated with hemodialysis by catheter or peritoneal dialysis compared with arteriovenous (AV) access were estimated with Fine and Gray models.
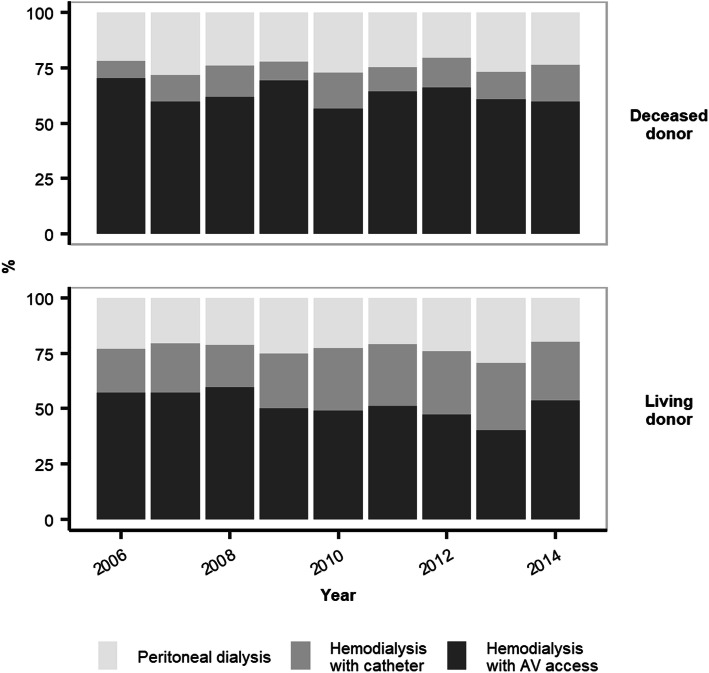
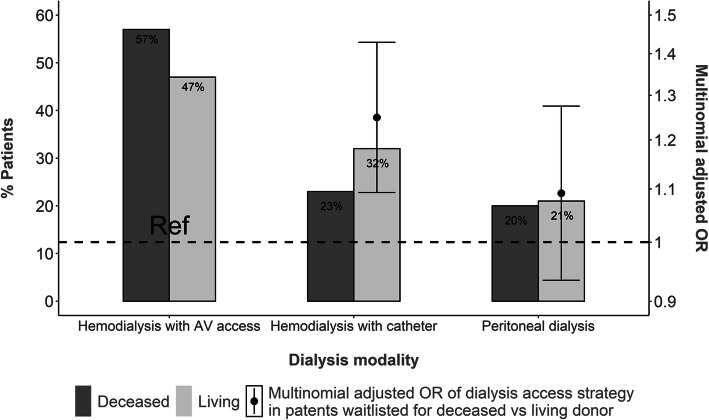
Living-donor candidates used pretransplant peritoneal dialysis at rates similar to deceased-donor KT candidates, but had significantly more frequent catheter than AV access for hemodialysis (adjusted OR 1.25; 95%CI 1.09-1.43). Over a median follow-up of 43 (IQR: 23-67) months, 6063 patients received transplants and 305 died before KT. Median duration of pretransplant dialysis was 15 (7-27) months for deceased-donor recipients and 9 (5-15) for living-donor recipients. Catheter use in deceased-donor candidates was associated with a lower SHR for KT (0.88, 95%CI 0.82-0.94) and a higher SHR for death (1.53, 95%CI 1.14-2.04). Only five deaths occurred in living-donor candidates, three of them with catheter use.
Pretransplant dialysis duration may be quite long even when planned with a living donor. Advantages from protecting these patients from AV fistula creation must be carefully evaluated against catheter-related risks.
对于终末期肾病患者来说,早期进行肾移植是最佳选择,但对于在此背景下的透析通路策略,人们知之甚少。我们研究了根据供体来源,等待早期肾移植的成年患者的透析通路实践模式及其与结局的关系。
本研究来自 REIN 登记处(2002-2014 年),纳入了 9331 名在开始透析前或开始透析后 6 个月内等待肾移植的新透析患者(年龄 18-69 岁):8342 名候选者接受了已故供体肾移植,989 名接受了活体供体肾移植。使用 Fine-Gray 模型估计与动静脉(AV)通路相比,通过导管或腹膜透析的血液透析的肾移植和死亡的亚分布风险比(SHR)。
活体供体候选者接受移植前腹膜透析的比例与已故供体肾移植候选者相似,但接受血液透析时导管的比例明显高于 AV 通路(校正比值比 1.25;95%CI 1.09-1.43)。在中位随访 43(IQR:23-67)个月期间,6063 名患者接受了移植,305 名患者在移植前死亡。已故供体受者的移植前透析中位时间为 15(7-27)个月,活体供体受者为 9(5-15)个月。已故供体候选者使用导管与肾移植 SHR 降低(0.88,95%CI 0.82-0.94)和死亡 SHR 升高(1.53,95%CI 1.14-2.04)相关。活体供体候选者仅发生了 5 例死亡,其中 3 例与导管使用有关。
即使计划使用活体供体,移植前的透析时间也可能相当长。必须仔细评估保护这些患者免受动静脉瘘创建的益处与导管相关风险的关系。