Tillmann Taavi, Läll Kristi, Dukes Oliver, Veronesi Giovanni, Pikhart Hynek, Peasey Anne, Kubinova Ruzena, Kozela Magdalena, Pajak Andrzej, Nikitin Yuri, Malyutina Sofia, Metspalu Andres, Esko Tõnu, Fischer Krista, Kivimäki Mika, Bobak Martin
Department of Epidemiology & Public Health, University College London, 1-19 Torrington Place, London WC1E 7HB, UK.
Centre for Non-Communicable Disease, Institute for Global Health, University College London, 30 Guilford Street, London WC1N 1EH, UK.
Eur Heart J. 2020 Sep 14;41(35):3325-3333. doi: 10.1093/eurheartj/ehaa571.
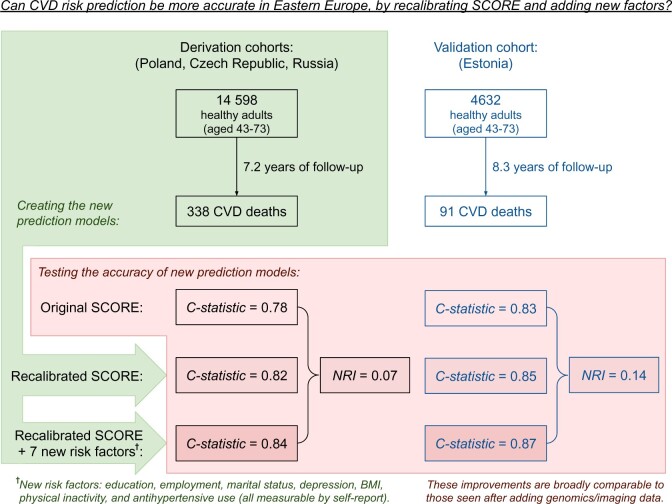
Cardiovascular disease (CVD) risk prediction models are used in Western European countries, but less so in Eastern European countries where rates of CVD can be two to four times higher. We recalibrated the SCORE prediction model for three Eastern European countries and evaluated the impact of adding seven behavioural and psychosocial risk factors to the model.
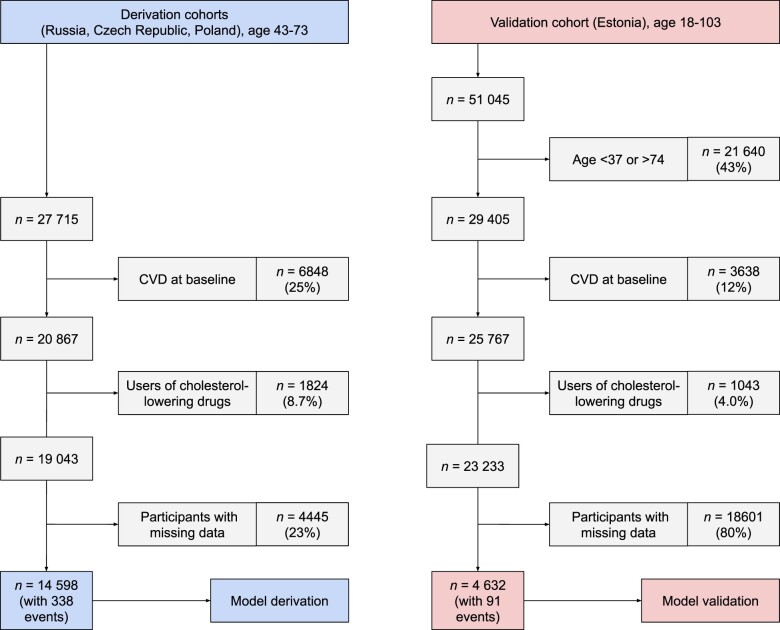
We developed and validated models using data from the prospective HAPIEE cohort study with 14 598 participants from Russia, Poland, and the Czech Republic (derivation cohort, median follow-up 7.2 years, 338 fatal CVD cases) and Estonian Biobank data with 4632 participants (validation cohort, median follow-up 8.3 years, 91 fatal CVD cases). The first model (recalibrated SCORE) used the same risk factors as in the SCORE model. The second model (HAPIEE SCORE) added education, employment, marital status, depression, body mass index, physical inactivity, and antihypertensive use. Discrimination of the original SCORE model (C-statistic 0.78 in the derivation and 0.83 in the validation cohorts) was improved in recalibrated SCORE (0.82 and 0.85) and HAPIEE SCORE (0.84 and 0.87) models. After dichotomizing risk at the clinically meaningful threshold of 5%, and when comparing the final HAPIEE SCORE model against the original SCORE model, the net reclassification improvement was 0.07 [95% confidence interval (CI) 0.02-0.11] in the derivation cohort and 0.14 (95% CI 0.04-0.25) in the validation cohort.
Our recalibrated SCORE may be more appropriate than the conventional SCORE for some Eastern European populations. The addition of seven quick, non-invasive, and cheap predictors further improved prediction accuracy.
心血管疾病(CVD)风险预测模型在西欧国家得到应用,但在CVD发病率可能高出两到四倍的东欧国家应用较少。我们对三个东欧国家的SCORE预测模型进行了重新校准,并评估了在该模型中加入七个行为和心理社会风险因素的影响。
我们利用前瞻性HAPIEE队列研究的数据开发并验证了模型,该研究有来自俄罗斯、波兰和捷克共和国的14598名参与者(推导队列,中位随访7.2年,338例致命性CVD病例),以及爱沙尼亚生物银行数据中的4632名参与者(验证队列,中位随访8.3年,91例致命性CVD病例)。第一个模型(重新校准的SCORE)使用与SCORE模型相同的风险因素。第二个模型(HAPIEE SCORE)加入了教育程度、就业情况、婚姻状况、抑郁、体重指数、缺乏身体活动和抗高血压药物使用情况。原SCORE模型的辨别能力(推导队列中的C统计量为0.78,验证队列中为0.83)在重新校准的SCORE(0.82和0.85)和HAPIEE SCORE(0.84和0.87)模型中得到了改善。在将风险在具有临床意义的5%阈值处进行二分后,当将最终的HAPIEE SCORE模型与原SCORE模型进行比较时,推导队列中的净重新分类改善为0.07 [95%置信区间(CI)0.02 - 0.11],验证队列中为0.14(95% CI 0.04 - 0.25)。
对于一些东欧人群,我们重新校准的SCORE可能比传统的SCORE更合适。加入七个快速、非侵入性且廉价的预测因素进一步提高了预测准确性。