Zeljković Ivan, Bulj Nikola, Kordić Krešimir, Pavlović Nikola, Radeljić Vjekoslav, Benko Ivica, Zadro Kordić Ines, Đula Kristijan, Kos Nikola, Delić Brkljačić Diana, Manola Šime
Department of Cardiology, Sestre milosrdnice University Hospital Centre, Zagreb, Croatia.
School of Medicine, University of Zagreb, Zagreb, Croatia.
Int J Cardiol Heart Vasc. 2020 Sep 25;31:100642. doi: 10.1016/j.ijcha.2020.100642. eCollection 2020 Dec.
Although there are numerous studies reflecting predictors of atrial fibrillation (AF) recurrence (AFR) after pulmonary vein isolation (PVI), data on atrial appendages' mechanics is scarce. This study aimed to assess atrial appendages' mechanics by 2-dimensional (2D) and 3-dimenssional (3D) transoesphageal echocardiography (TEE) and to explore its value to predict AFR after PVI.
Consecutive patients with paroxysmal AF undergoing first PVIwere analysed. 3D and 2D-TEE with tissue Doppler imaging (TDI) and strain analysis was obtained prior to the PVI, including: left atrial appendage (LAA) TDI and strain analysis, LAA ostium surface area, right atrial appendage's TDI velocity and superior vena cava (SVC) ostium surface area. The primary end-point was freedom from any documented recurrence of atrial arrhythmia lasting > 30 s
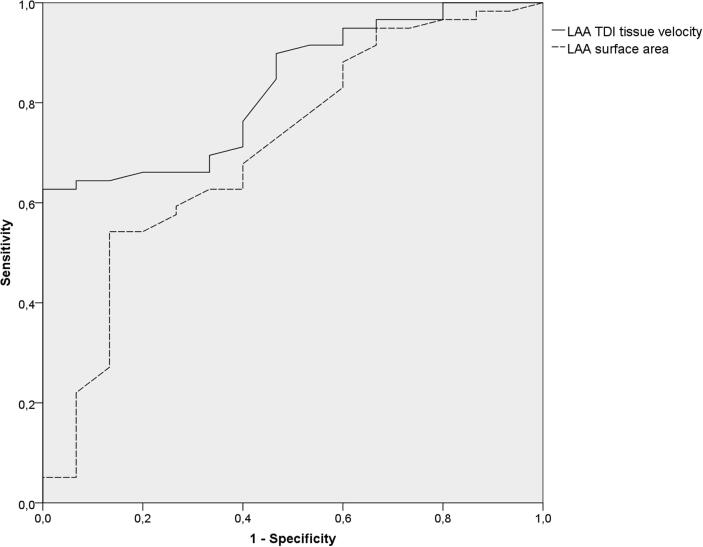
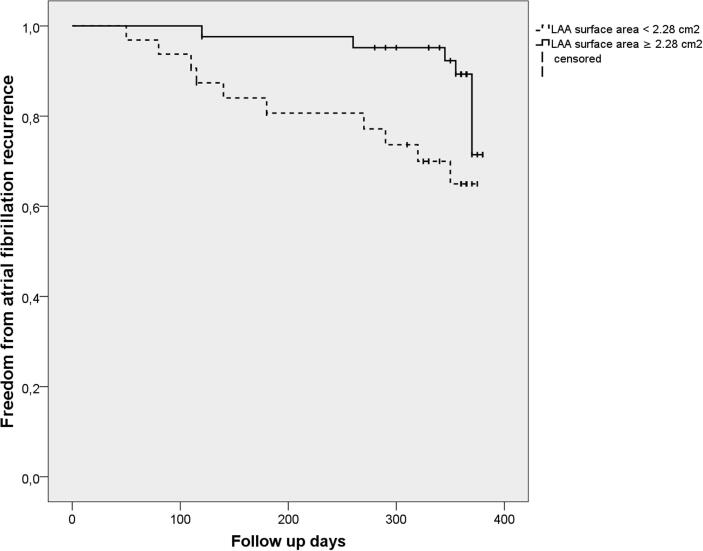
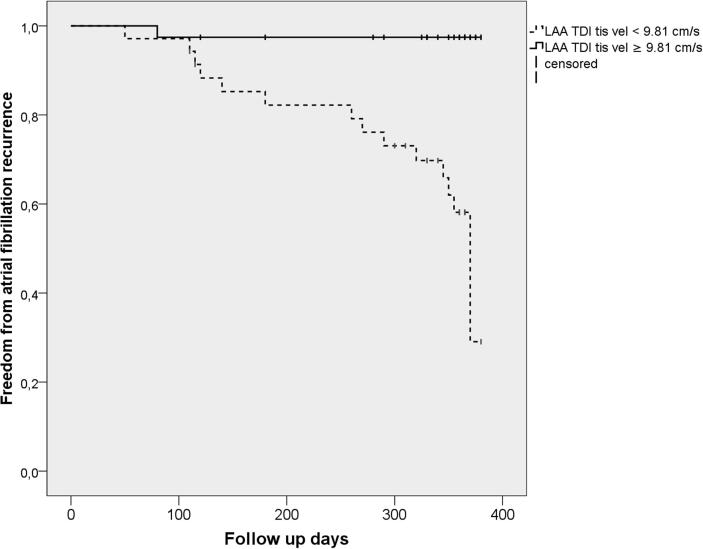
This single-centre, prospective study included 74 patients with paroxysmal AF (median age 59 years; 36% female; BMI 27.4 ± 4.1 kg/m, LA volume index 32 ± 11 mL/m). After a median follow-up of 14 (IQR 10-22) months, 21 (28%) patients had AFR. In a univariate and multivariate Cox-regression analysis LAA TDI velocity (HR 1.48, 95%CI 1.28-1.62, p < 0.001) and LAA ostium surface area(HR 1.58, 95%CI 1.06-1.81, p = 0.033) both independently predicted AFR after single PVI. RAA TDI velocity and SVC ostium surface area were not correlated to AFR.
Paroxysmal AF patients with lower LAA TDI tissue velocity and LAA ostium surface area have higher risk of developing AFR after PVI. To our knowledge, this is the first study assessing atrial appendages' mechanics in predicting AFR after PVI.Clinical trial registration: www.drks.de(Identifier: DRKS00010495).
尽管有大量研究反映了肺静脉隔离(PVI)后房颤(AF)复发(AFR)的预测因素,但关于心耳力学的数据却很少。本研究旨在通过二维(2D)和三维(3D)经食管超声心动图(TEE)评估心耳力学,并探讨其预测PVI后AFR的价值。
对连续接受首次PVI的阵发性AF患者进行分析。在PVI之前获得3D和2D-TEE以及组织多普勒成像(TDI)和应变分析,包括:左心耳(LAA)TDI和应变分析、LAA口面积、右心耳的TDI速度和上腔静脉(SVC)口面积。主要终点是无任何记录的持续时间>30秒的房性心律失常复发。
这项单中心前瞻性研究纳入了74例阵发性AF患者(中位年龄59岁;36%为女性;BMI 27.4±4.1kg/m²,左房容积指数32±11mL/m²)。中位随访14(IQR 10 - 22)个月后,21例(28%)患者发生AFR。在单因素和多因素Cox回归分析中,LAA TDI速度(HR 1.48,95%CI 1.28 - 1.62,p<0.001)和LAA口面积(HR 1.58,95%CI 1.06 - 1.81,p = 0.033)均独立预测单次PVI后的AFR。右心耳TDI速度和SVC口面积与AFR无关。
LAA TDI组织速度和LAA口面积较低的阵发性AF患者在PVI后发生AFR的风险较高。据我们所知,这是第一项评估心耳力学在预测PVI后AFR方面的研究。临床试验注册:www.drks.de(标识符:DRKS00010495)。