Department of Pediatrics, Alberta Children's Hospital, University of Calgary, Calgary, AB, Canada.
Department of Nutrition, Georgia State University, Atlanta, GA, USA.
Diabetologia. 2021 Jan;64(1):119-128. doi: 10.1007/s00125-020-05287-1. Epub 2020 Oct 7.
AIMS/HYPOTHESIS: The aim of this work was to examine the relationship between family history of type 1 diabetes, birthweight, growth during the first 2 years and development of multiple beta cell autoantibodies in children with a first-degree relative with type 1 diabetes and HLA-conferred disease susceptibility.
In a secondary analysis of the Trial to Reduce IDDM in the Genetically at Risk (TRIGR), clinical characteristics and development of beta cell autoantibodies were compared in relation to family history of type 1 diabetes (mother vs father vs sibling) in 2074 children from families with a single affected family member.
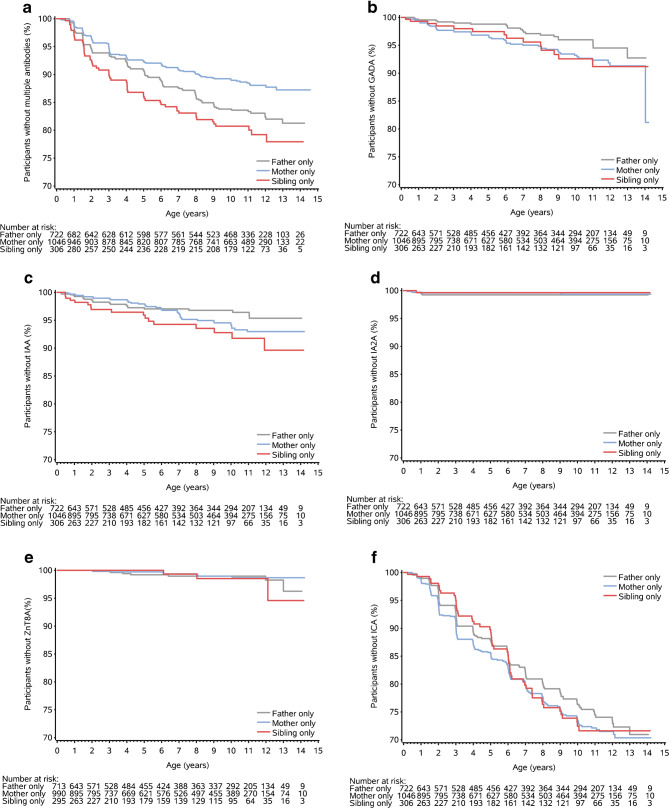
Multiple autoantibodies (≥2 of 5 measured) developed in 277 (13%) children: 107 (10%), 114 (16%) and 56 (18%) born with a mother, father or sibling with type 1 diabetes, respectively (p < 0.001). The HR for time to multiple autoimmunity was 0.54 (95% CI 0.39, 0.75) in offspring of affected mothers (n = 107/1046, p < 0.001) and 0.81 (95% CI 0.59, 1.11) (n = 114/722, p = 0.19) in offspring of affected fathers, compared with participants with a sibling with type 1 diabetes (comparator group n = 56/306). The time to the first autoantibody present (to insulin, GAD, tyrosine phosphatase-related insulinoma-associated 2 molecules, islet cell or zinc transporter 8) was similar in the three groups. Height velocity (z score/year) in the first 24 months was independently associated with developing multiple antibodies in the total cohort (HR 1.31 [95% CI 1.01, 1.70], p = 0.04). A higher birthweight in children born to an affected mother vs affected father or an affected sibling was not related to the risk of multiple autoimmunity.
CONCLUSIONS/INTERPRETATION: The risk of developing multiple autoantibodies was lower in children with maternal type 1 diabetes. For the whole group, this risk of developing multiple autoantibodies was independent of birthweight but was greater in those with increased height velocity during the first 2 years of life. However, the risk associated with paternal type 1 diabetes was not linked to differences in birthweight or early growth.
ClinicalTrials.gov NCT00179777 Graphical abstract.
目的/假设:本研究旨在探讨一级亲属中患有 1 型糖尿病的个体的家族史、出生体重、前 2 年的生长情况以及多种胰岛β细胞自身抗体的发展之间的关系,这些个体具有 1 型糖尿病和 HLA 赋予的疾病易感性。
在遗传易感性 1 型糖尿病的降低试验(TRIGR)的二次分析中,比较了来自单一致病家族的 2074 名儿童的临床特征和胰岛β细胞自身抗体的发展与 1 型糖尿病家族史(母亲与父亲与兄弟姐妹)之间的关系。
277 名儿童(13%)出现多种自身抗体(≥5 项测量指标中的 2 项):分别有 107 名(10%)、114 名(16%)和 56 名(18%)出生时母亲、父亲或兄弟姐妹患有 1 型糖尿病(p<0.001)。患有 1 型糖尿病的母亲的后代(n=107/1046)发生多种自身免疫的 HR 为 0.54(95%CI 0.39,0.75)(p<0.001),而患有 1 型糖尿病的父亲的后代(n=114/722)的 HR 为 0.81(95%CI 0.59,1.11)(p=0.19),与患有 1 型糖尿病兄弟姐妹的参与者相比(对照组 n=56/306)。三组中首次出现自身抗体(胰岛素、GAD、酪氨酸磷酸酶相关胰岛素瘤相关 2 分子、胰岛细胞或锌转运蛋白 8)的时间相似。在整个队列中,前 24 个月的身高增长速度(z 评分/年)与发展多种抗体独立相关(HR 1.31[95%CI 1.01,1.70],p=0.04)。与母亲患有 1 型糖尿病的儿童相比,出生体重较高与母亲患有 1 型糖尿病或父亲患有 1 型糖尿病或兄弟姐妹患有 1 型糖尿病的儿童发生多种自身免疫的风险无相关性。
结论/解释:患有 1 型糖尿病的母亲的孩子发生多种自身抗体的风险较低。对于整个群体,发展多种自身抗体的风险与出生体重无关,但在生命的前 2 年身高增长较快的儿童中风险更大。然而,与父亲患有 1 型糖尿病相关的风险与出生体重或早期生长的差异无关。
ClinicalTrials.gov NCT00179777 图摘要。