Endres Paul, Rosovsky Rachel, Zhao Sophia, Krinsky Scott, Percy Shananssa, Kamal Omer, Roberts Russel J, Lopez Natasha, Sise Meghan E, Steele David J R, Lundquist Andrew L, Rhee Eugene P, Hibbert Kathryn A, Hardin C Corey, Mc Causland Finnian R, Czarnecki Peter G, Mutter Walter, Tolkoff-Rubin Nina, Allegretti Andrew S
Division of Nephrology, Department of Medicine, Massachusetts General Hospital, 55 Fruit Street, GRB 1008, Boston, MA, 02114, USA.
Division of Hematology, Department of Medicine, Massachusetts General Hospital, Boston, MA, USA.
J Thromb Thrombolysis. 2021 May;51(4):966-970. doi: 10.1007/s11239-020-02301-6. Epub 2020 Oct 7.
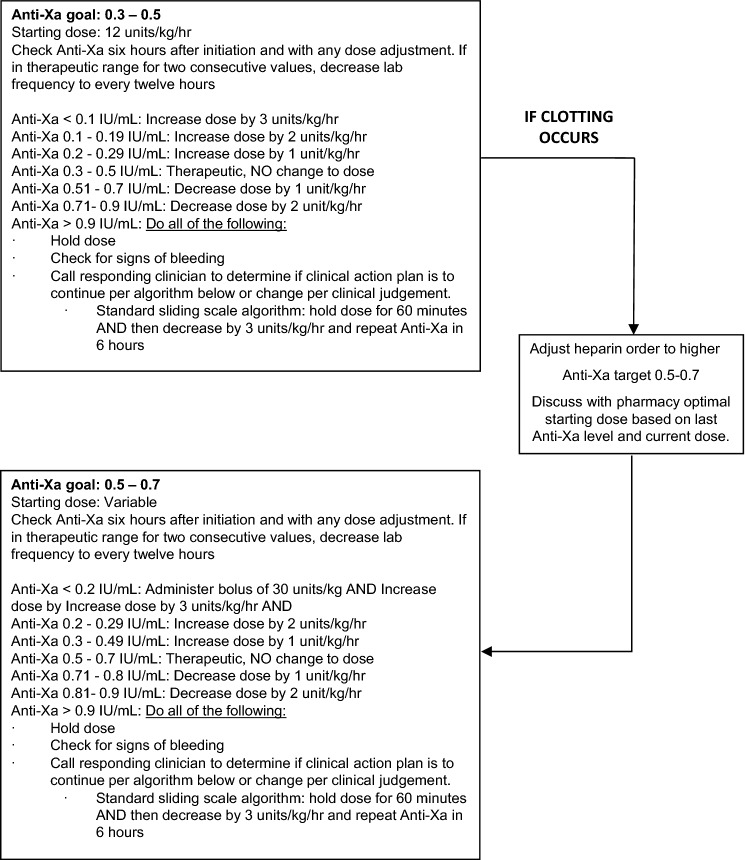
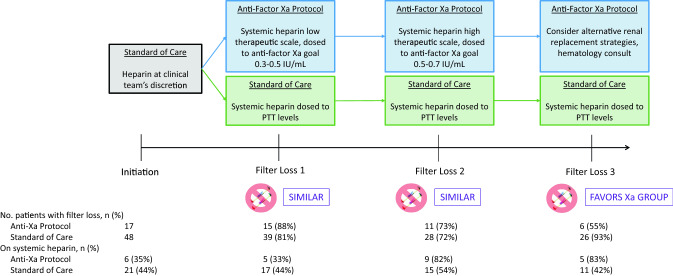
Coronavirus disease 2019 (COVID-19) appears to be associated with increased arterial and venous thromboembolic disease. These presumed abnormalities in hemostasis have been associated with filter clotting during continuous renal replacement therapy (CRRT). We aimed to characterize the burden of CRRT filter clotting in COVID-19 infection and to describe a CRRT anticoagulation protocol that used anti-factor Xa levels for systemic heparin dosing. Multi-center study of consecutive patients with COVID-19 receiving CRRT. Primary outcome was CRRT filter loss. Sixty-five patients were analyzed, including 17 using an anti-factor Xa protocol to guide systemic heparin dosing. Fifty-four out of 65 patients (83%) lost at least one filter. Median first filter survival time was 6.5 [2.5, 33.5] h. There was no difference in first or second filter loss between the anti-Xa protocol and standard of care anticoagulation groups, however fewer patients lost their third filter in the protocolized group (55% vs. 93%) resulting in a longer median third filter survival time (24 [15.1, 54.2] vs. 17.3 [9.5, 35.1] h, p = 0.04). The rate of CRRT filter loss is high in COVID-19 infection. An anticoagulation protocol using systemic unfractionated heparin, dosed by anti-factor Xa levels is reasonable approach to anticoagulation in this population.
2019冠状病毒病(COVID-19)似乎与动静脉血栓栓塞性疾病的增加有关。这些推测的止血异常与持续肾脏替代治疗(CRRT)期间滤器凝血有关。我们旨在描述COVID-19感染中CRRT滤器凝血的负担,并描述一种使用抗Xa因子水平来调整全身肝素剂量的CRRT抗凝方案。对接受CRRT的COVID-19连续患者进行多中心研究。主要结局是CRRT滤器丢失。分析了65例患者,其中17例使用抗Xa因子方案指导全身肝素剂量调整。65例患者中有54例(83%)至少丢失了一个滤器。首个滤器的中位生存时间为6.5[2.5, 33.5]小时。抗Xa方案组与标准护理抗凝组在首个或第二个滤器丢失方面没有差异,然而,在方案组中丢失第三个滤器的患者较少(55%对93%),导致第三个滤器的中位生存时间更长(24[15.1, 54.2]对17.3[9.5, 35.1]小时,p = 0.04)。COVID-19感染中CRRT滤器丢失率很高。使用普通肝素全身给药并根据抗Xa因子水平调整剂量的抗凝方案是该人群抗凝的合理方法。