Department of Surgery, Faculty of Medicine, The University of British Columbia, Vancouver, British Columbia, Canada.
Department of Statistics, Faculty of Science, The University of British Columbia, Vancouver, British Columbia, Canada.
JAMA Otolaryngol Head Neck Surg. 2020 Dec 1;146(12):1149-1155. doi: 10.1001/jamaoto.2020.3147.
High local recurrence rates with aggressive disease remain the main concern in oral cancer survival. Use of a translational device using fluorescence visualization (FV) approved by the US Food and Drug Administration and Health Canada, has shown a marked reduction in the 3-year local recurrence rate of high-grade oral lesions in a single-center observational study.
To determine whether FV- guided surgery can improve local control rates in the treatment of in situ or T1 to T2 category oral squamous cell carcinoma (OSCC).
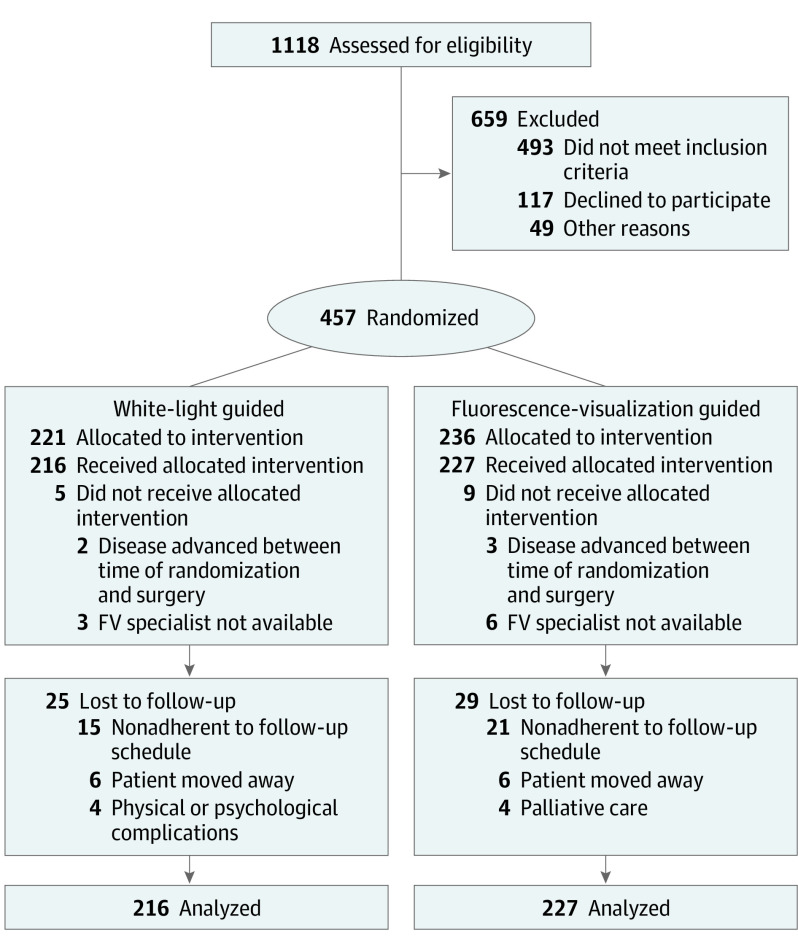
DESIGN, SETTING, AND PARTICIPANTS: A multicenter randomized clinical trial was conducted in a surgical setting. A total of 457 patients were enrolled between January 18, 2010, and April 30, 2015. Data analysis of the intention-to-treat population was performed from April 3, 2019, to March 20, 2020. Patients with histologically confirmed high-grade dysplasia/carcinoma in situ or T1 to T2 category OSCC were randomized to receive traditional peroral surgery or FV-guided surgery.
Fluorescence visualization during surgery.
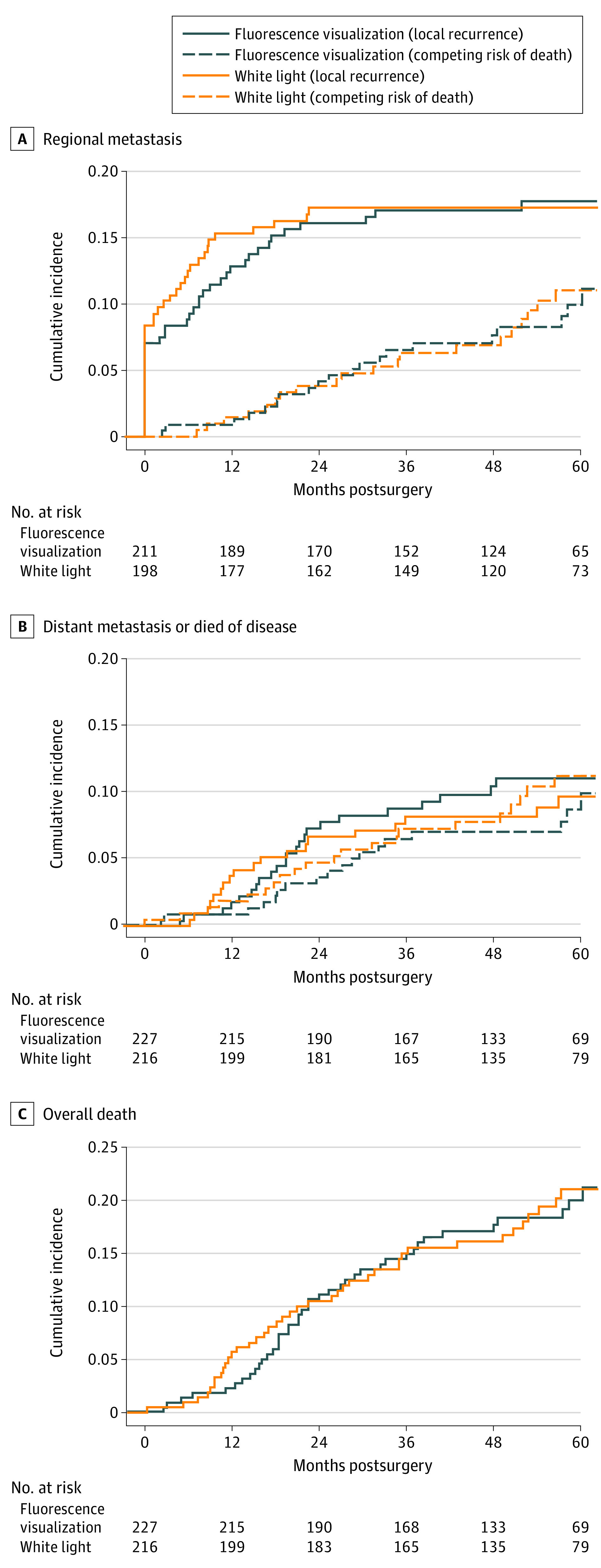
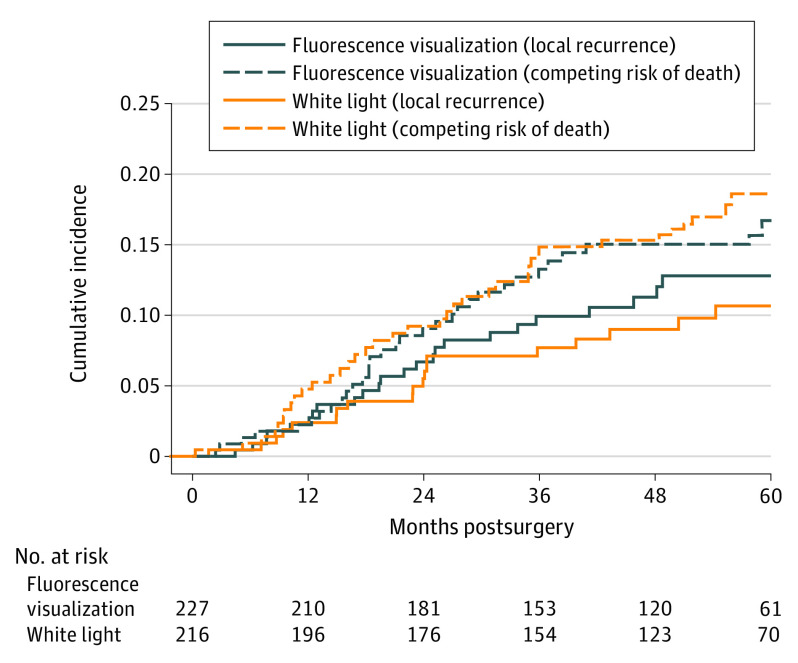
The primary outcome was local recurrence of OSCC. Secondary outcomes were failure of the first-pass margin, defined as a histologically confirmed positive margin for severe dysplasia or greater histologic change of the main specimen (ie, not the margins taken from the resection bed), regional or distant metastasis, and death due to disease.
Of the 457 patients enrolled in the study, 443 patients (264 [59.6%] men; mean [SD] age, 61.5 [13.3] years) completed the randomized treatment: 227 FV-guided and 216 non-FV guided surgery. The median follow-up was 52 (range, 0.29-90.8) months. In total, 45 patients (10.2%) experienced local recurrence. The 3-year local recurrence rate was 9.4% in the FV-guided group and 7.2% in the non-FV group (difference, 2.2%; 95% CI, -3.2% to 7.4%). Other similarities between the FV vs non-FV groups included failure of first-pass margin (68/227 [30.0%]) vs 65/216 [30.1%]), regional failure (39/227 [17.2%] vs 37/216 [17.1%]), disease-specific survival (23/227 [10.1%] vs 19/26 [8.8%]), and overall survival (41/227 [18.1%] vs 38/216 [17.6%]) were also similar between groups. No adverse events were judged to be related to the intervention.
In this randomized clinical trial, FV-guided surgery did not improve local control rates in the treatment of patients with in situ or T1 to T2 category oral cancer. Under a controlled environment, FV-guided surgery did not have an evident effect in reduction of local recurrence for localized OSCC. This result suggests that attention be directed to strategies other than improving definitions of nonapparent disease at clinical margins to identify the sources of local recurrence.
ClinicalTrial.gov Identifier: NCT01039298.
重要性:在口腔癌的生存中,高局部复发率和侵袭性疾病仍然是主要关注点。使用美国食品和药物管理局和加拿大卫生部批准的翻译设备(荧光可视化[FV]),在一项单中心观察性研究中,已显示出高级别口腔病变的 3 年局部复发率显著降低。
目的:确定 FV 引导手术是否可以改善原位或 T1 至 T2 类口腔鳞状细胞癌(OSCC)的局部控制率。
设计、地点和参与者:在手术环境中进行了一项多中心随机临床试验。2010 年 1 月 18 日至 2015 年 4 月 30 日期间共纳入 457 例患者。对意向治疗人群进行数据分析的时间为 2019 年 4 月 3 日至 2020 年 3 月 20 日。将组织学证实为高级别发育不良/原位癌或 T1 至 T2 类 OSCC 的患者随机分为接受传统经口手术或 FV 引导手术。
干预措施:手术过程中的荧光可视化。
主要结果和措施:主要结局是 OSCC 的局部复发。次要结局是首次通过边缘失败,定义为主要标本的组织学证实阳性边缘(即不是从切除床获得的边缘),区域或远处转移,以及疾病相关死亡。
结果:在这项研究中,共纳入 457 例患者,443 例患者(264 [59.6%] 名男性;平均[SD]年龄 61.5 [13.3] 岁)完成了随机治疗:227 例 FV 引导和 216 例非 FV 引导手术。中位随访时间为 52 个月(范围,0.29-90.8)。共有 45 例(10.2%)患者出现局部复发。FV 引导组的 3 年局部复发率为 9.4%,非 FV 组为 7.2%(差异 2.2%;95%CI,-3.2%至 7.4%)。FV 与非 FV 组之间的其他相似之处还包括首次通过边缘失败(68/227 [30.0%])与 65/216 [30.1%])、区域失败(39/227 [17.2%])与 37/216 [17.1%])、疾病特异性生存率(23/227 [10.1%])与 19/26 [8.8%])和总生存率(41/227 [18.1%])也相似。没有不良事件被认为与干预有关。
结论和相关性:在这项随机临床试验中,FV 引导手术并未提高原位或 T1 至 T2 类口腔癌患者的局部控制率。在受控环境下,FV 引导手术在降低局部复发率方面对局限性 OSCC 没有明显作用。这一结果表明,需要关注的是在临床边缘改善非明显疾病的定义之外的策略,以确定局部复发的来源。
试验注册:ClinicalTrials.gov 标识符:NCT01039298。