Division of Infectious Diseases, Department of Internal Medicine, University of Utah, Salt Lake City, UT, United States of America.
Division of Pediatric Infectious Diseases, Department of Pediatrics, University of Utah, Salt Lake City, UT, United States of America.
PLoS Negl Trop Dis. 2020 Oct 9;14(10):e0008677. doi: 10.1371/journal.pntd.0008677. eCollection 2020 Oct.
Diarrhea is one of the leading causes of childhood morbidity and mortality in lower- and middle-income countries. In such settings, access to laboratory diagnostics are often limited, and decisions for use of antimicrobials often empiric. Clinical predictors are a potential non-laboratory method to more accurately assess diarrheal etiology, the knowledge of which could improve management of pediatric diarrhea.
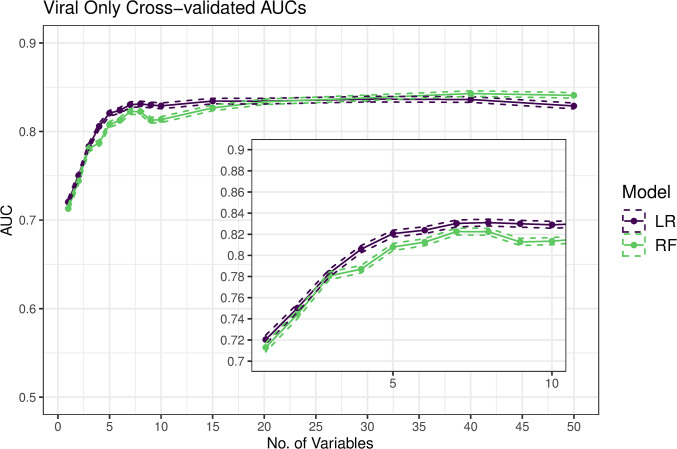
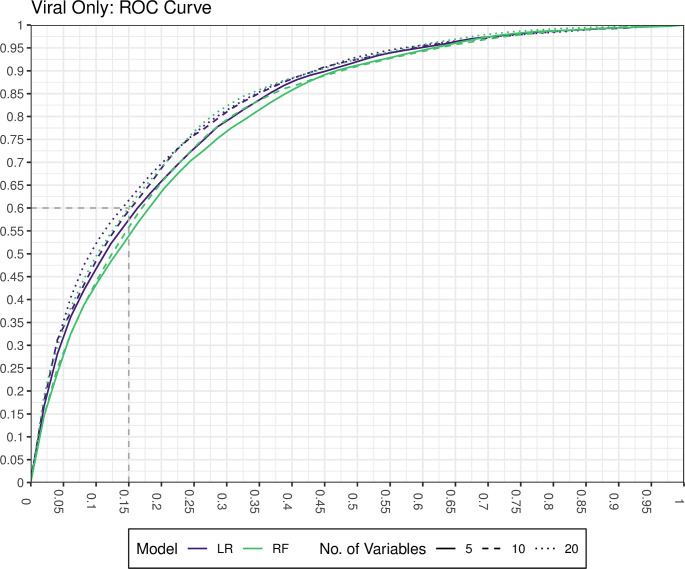
We used clinical and quantitative molecular etiologic data from the Global Enteric Multicenter Study (GEMS), a prospective, case-control study, to develop predictive models for the etiology of diarrhea. Using random forests, we screened the available variables and then assessed the performance of predictions from random forest regression models and logistic regression models using 5-fold cross-validation.
We identified 1049 cases where a virus was the only etiology, and developed predictive models against 2317 cases where the etiology was known but non-viral (bacterial, protozoal, or mixed). Variables predictive of a viral etiology included lower age, a dry and cold season, increased height-for-age z-score (HAZ), lack of bloody diarrhea, and presence of vomiting. Cross-validation suggests an AUC of 0.825 can be achieved with a parsimonious model of 5 variables, achieving a specificity of 0.85, a sensitivity of 0.59, a NPV of 0.82 and a PPV of 0.64.
Predictors of the etiology of pediatric diarrhea can be used by providers in low-resource settings to inform clinical decision-making. The use of non-laboratory methods to diagnose viral causes of diarrhea could be a step towards reducing inappropriate antibiotic prescription worldwide.
腹泻是中低收入国家儿童发病率和死亡率的主要原因之一。在这些环境中,通常无法获得实验室诊断,并且对抗生素的使用决策往往是经验性的。临床预测因子是一种潜在的非实验室方法,可以更准确地评估腹泻病因,了解这些方法可以改善儿科腹泻的管理。
我们使用了全球肠道多中心研究(GEMS)的临床和定量分子病因数据,这是一项前瞻性病例对照研究,以开发针对腹泻病因的预测模型。我们使用随机森林筛选可用变量,然后使用 5 折交叉验证评估随机森林回归模型和逻辑回归模型的预测性能。
我们确定了 1049 例病毒是唯一病因的病例,并针对已知但非病毒病因(细菌、原生动物或混合)的 2317 例病例开发了预测模型。预测病毒病因的变量包括年龄较小、干燥寒冷的季节、身高年龄 Z 分数(HAZ)增加、无血性腹泻和呕吐。交叉验证表明,使用 5 个变量的简约模型可以达到 0.825 的 AUC,特异性为 0.85,敏感性为 0.59,NPV 为 0.82,PPV 为 0.64。
在资源匮乏的环境中,提供者可以使用腹泻病因的预测因子来为临床决策提供信息。使用非实验室方法诊断腹泻的病毒病因可能是减少全球不合理使用抗生素的一步。