Nijman Ruud G, Jorgensen Rikke, Levin Michael, Herberg Jethro, Maconochie Ian K
Department of Paediatric Accident and Emergency, St. Mary's Hospital - Imperial College NHS Healthcare Trust, London, United Kingdom.
Section of Paediatric Infectious Diseases, Department of Infectious Diseases, Faculty of Medicine, Imperial College London, London, United Kingdom.
Front Pediatr. 2020 Sep 17;8:548154. doi: 10.3389/fped.2020.548154. eCollection 2020.
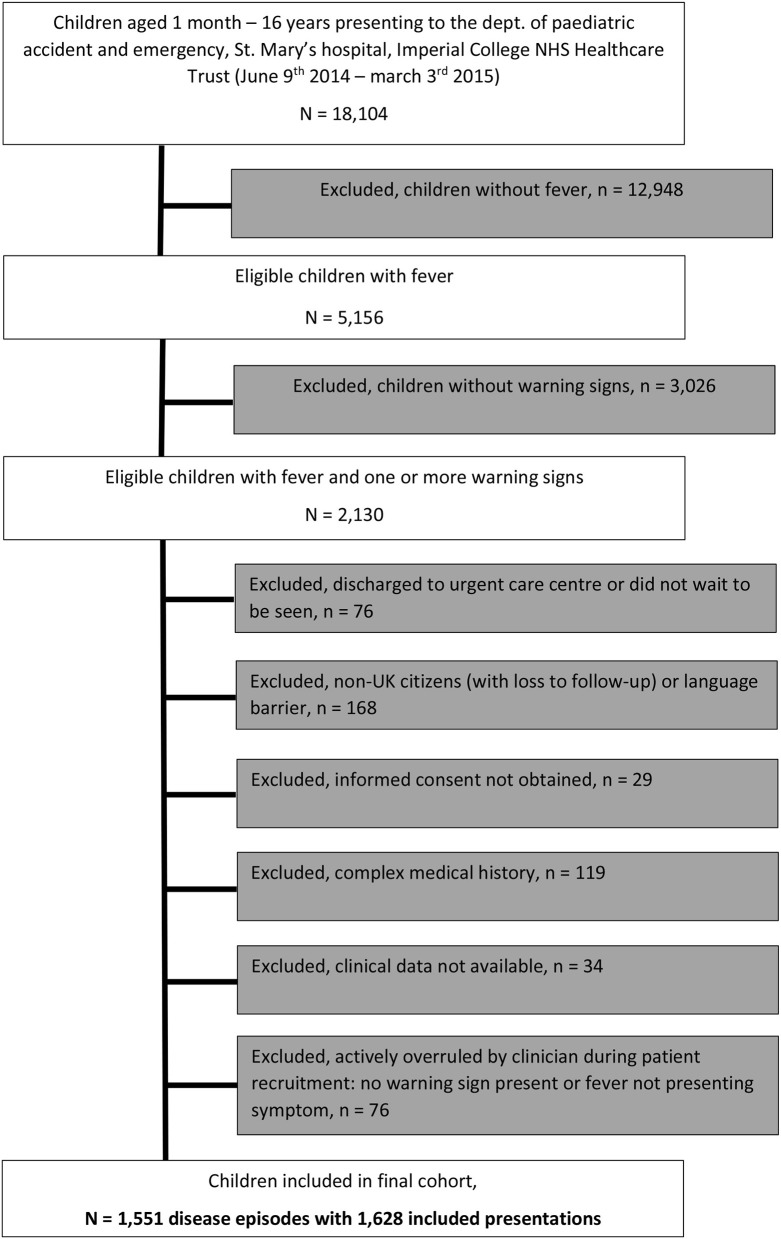
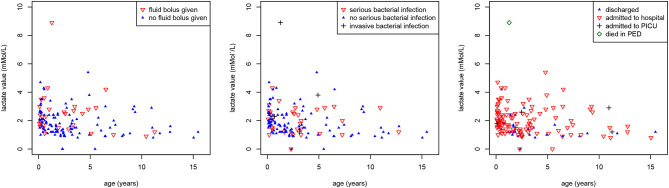
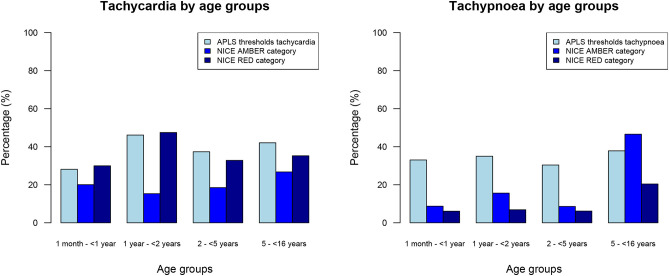
To study warning signs of serious infections in febrile children presenting to PED, ascertain their risk of having sepsis, and evaluate their management. Prospective observational study. A single pediatric emergency department (PED). Febrile children, aged 1 month-16 years, with >= 1 warning signs of sepsis. Clinical characteristics, including different thresholds for tachycardia and tachypnoea, and their association with (1) delivery of pediatric sepsis 6 (PS6) interventions, (2) final diagnosis of invasive bacterial infection (IBI), (3) the risk for pediatric intensive care unit (PICU) admission, and (4) death. Forty-one percent of 5,156 febrile children had warning signs of sepsis. 1,606 (34%) children had tachypnoea and 1,907 (39%) children had tachycardia when using APLS threshold values. Using the NICE sepsis guidelines thresholds resulted in 1,512 (32%) children having tachypnoea (kappa 0.56) and 2,769 (57%) children having tachycardia (kappa 0.66). Of 1,628 PED visits spanning 1,551 disease episodes, six children (0.4%) had IBI, with one death (0.06%), corresponding with 256 children requiring escalation of care according to sepsis guideline recommendations for each child with IBI. There were five additional PICU admissions (0.4%). 121 (7%) had intravenous antibiotics in PED; 39 children (2%) had an intravenous fluid bolus, inotrope drugs were started in one child. 440 children (27%) were reviewed by a senior clinician. In 4/11 children with IBI or PICU admission or death, PS6 interventions were delivered within 60 min after arriving. 1,062 (65%) visits had no PS6 interventions. Diagnostic performance of vital signs or sepsis criteria for predicting serious illness yielded a large proportion of false positives. Lactataemia was not associated with giving iv fluid boluses ( = 0.19) or presence of serious bacterial infections ( = 0.128). Many febrile children (41%) present with warning signs for sepsis, with only few of them undergoing investigations or treatment for true sepsis. Children with positive isolates in blood or CSF culture presented in a heterogeneous manner, with varying levels of urgency and severity of illness. Delivery of sepsis care can be improved in only a minority of children with IBI or admitted to PICU.
为研究儿科急诊(PED)中发热儿童严重感染的警示信号,确定其发生脓毒症的风险,并评估其治疗情况。进行前瞻性观察性研究。选取单一儿科急诊科(PED)。纳入年龄1个月至16岁、具有≥1个脓毒症警示信号的发热儿童。研究临床特征,包括心动过速和呼吸急促的不同阈值,以及它们与以下方面的关联:(1)儿科脓毒症6(PS6)干预措施的实施;(2)侵袭性细菌感染(IBI)的最终诊断;(3)儿科重症监护病房(PICU)收治风险;(4)死亡情况。5156名发热儿童中41%有脓毒症警示信号。采用APLS阈值时,1606名(34%)儿童有呼吸急促,1907名(39%)儿童有心动过速。采用英国国家卫生与临床优化研究所(NICE)脓毒症指南阈值时,1512名(32%)儿童有呼吸急促(kappa值为0.56),2769名(57%)儿童有心动过速(kappa值为0.66)。在涵盖1551次疾病发作的1628次PED就诊中,6名儿童(0.4%)患有IBI,1名死亡(0.06%),这意味着每例患有IBI的儿童按照脓毒症指南建议有256名儿童需要加强治疗。另有5名儿童(0.4%)被收治入PICU。121名(7%)在PED接受了静脉抗生素治疗;39名儿童(2%)接受了静脉推注补液,1名儿童开始使用血管活性药物。440名儿童(27%)由资深临床医生进行了评估。在11例患有IBI或被收治入PICU或死亡的儿童中,4例在到达后60分钟内实施了PS6干预措施。1062次(65%)就诊未实施PS6干预措施。生命体征或脓毒症标准对预测严重疾病的诊断效能产生了大量假阳性结果。血乳酸水平与给予静脉推注补液(P = 0.19)或严重细菌感染的存在(P = 0.128)无关。许多发热儿童(41%)有脓毒症警示信号,但其中只有少数因真正的脓毒症接受检查或治疗。血培养或脑脊液培养分离出阳性菌株的儿童表现各异,疾病的紧急程度和严重程度各不相同。只有少数患有IBI或被收治入PICU的儿童的脓毒症治疗情况能够得到改善。