Division of Infectious Diseases II and Immunology, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy.
Department of Internal Medicine and Therapeutics, University of Pavia, Pavia, Italy.
Cell Mol Immunol. 2021 Mar;18(3):604-612. doi: 10.1038/s41423-020-00557-9. Epub 2020 Oct 15.
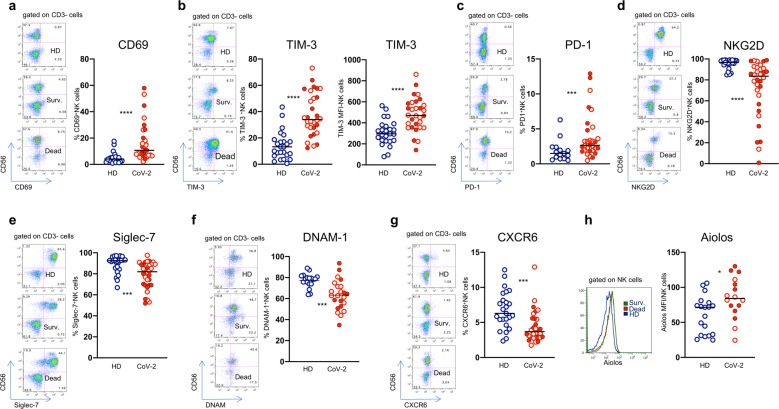
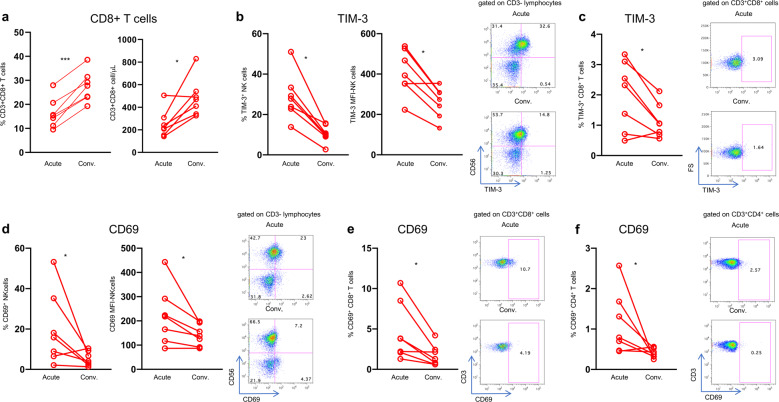
The relationship between severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and host immunity is poorly understood. We performed an extensive analysis of immune responses in 32 patients with severe COVID-19, some of whom succumbed. A control population of healthy subjects was included. Patients with COVID-19 had an altered distribution of peripheral blood lymphocytes, with an increased proportion of mature natural killer (NK) cells and low T-cell numbers. NK cells and CD8 T cells overexpressed T-cell immunoglobulin and mucin domain-3 (TIM-3) and CD69. NK cell exhaustion was attested by increased frequencies of programmed cell death protein 1 (PD-1) positive cells and reduced frequencies of natural killer group 2 member D (NKG2D)-, DNAX accessory molecule-1 (DNAM-1)- and sialic acid-binding Ig-like lectin 7 (Siglec-7)-expressing NK cells, associated with a reduced ability to secrete interferon (IFN)γ. Patients with poor outcome showed a contraction of immature CD56 and an expansion of mature CD57 FcεRIγ adaptive NK cells compared to survivors. Increased serum levels of IL-6 were also more frequently identified in deceased patients compared to survivors. Of note, monocytes secreted abundant quantities of IL-6, IL-8, and IL-1β which persisted at lower levels several weeks after recovery with concomitant normalization of CD69, PD-1 and TIM-3 expression and restoration of CD8 T cell numbers. A hyperactivated/exhausted immune response dominate in severe SARS-CoV-2 infection, probably driven by an uncontrolled secretion of inflammatory cytokines by monocytes. These findings unveil a unique immunological profile in COVID-19 patients that will help to design effective stage-specific treatments for this potentially deadly disease.
严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)与宿主免疫之间的关系尚未完全阐明。我们对 32 名重症 COVID-19 患者进行了广泛的免疫反应分析,其中一些患者死亡。纳入了健康受试者作为对照人群。COVID-19 患者外周血淋巴细胞分布发生改变,成熟自然杀伤(NK)细胞比例增加,T 细胞数量减少。NK 细胞和 CD8 T 细胞过度表达 T 细胞免疫球蛋白和粘蛋白结构域 3(TIM-3)和 CD69。NK 细胞衰竭表现为程序性细胞死亡蛋白 1(PD-1)阳性细胞频率增加,NK 细胞表达自然杀伤组 2 成员 D(NKG2D)、DNAX 辅助分子 1(DNAM-1)和唾液酸结合免疫球蛋白样凝集素 7(Siglec-7)的频率降低,与 IFNγ分泌能力降低有关。与幸存者相比,预后不良的患者表现为不成熟 CD56 的收缩和成熟 CD57 FcεRIγ适应性 NK 细胞的扩张。与幸存者相比,死亡患者的血清 IL-6 水平也升高。值得注意的是,与幸存者相比,单核细胞分泌大量的 IL-6、IL-8 和 IL-1β,这些细胞因子在恢复期后数周内仍以较低水平持续分泌,同时 CD69、PD-1 和 TIM-3 的表达正常化,CD8 T 细胞数量恢复。在严重的 SARS-CoV-2 感染中,过度激活/衰竭的免疫反应占主导地位,可能是由单核细胞不受控制地分泌炎症细胞因子所驱动。这些发现揭示了 COVID-19 患者独特的免疫学特征,有助于为这种潜在致命疾病设计有效的阶段特异性治疗方法。