Leisman Daniel E, Mastroianni Fiore, Fisler Grace, Shah Sareen, Hasan Zubair, Narasimhan Mangala, Taylor Matthew D, Deutschman Clifford S
Department of Medicine, Massachusetts General Hospital, Boston, MA.
Sepsis Research Laboratory, Feinstein Institute for Medical Research, Manhasset, NY.
Crit Care Explor. 2020 Sep 29;2(10):e0230. doi: 10.1097/CCE.0000000000000230. eCollection 2020 Oct.
To assess the early physiologic response to angiotensin-II treatment in patients with coronavirus disease 2019-induced respiratory failure and distributive shock.
Retrospective consecutive-sample cohort study.
Three medical ICUs in New York during the coronavirus disease 2019 outbreak.
All patients were admitted to the ICU with respiratory failure and were receiving norepinephrine for distributive shock.
The treatment groups were patients who received greater than or equal to 1 hour of angiotensin-II treatment. Time-zero was the time of angiotensin-II initiation. Controls were identified using a 2:1 hierarchical process that matched for 1) date and unit of admission; 2) specific organ support modalities; 3) age; 4) chronic lung, cardiovascular, and kidney disease; and 5) sex. Time-zero in the control group was 21 hours post vasopressor initiation, the mean duration of vasopressor therapy prior to angiotensin-II initiation in the treated group.
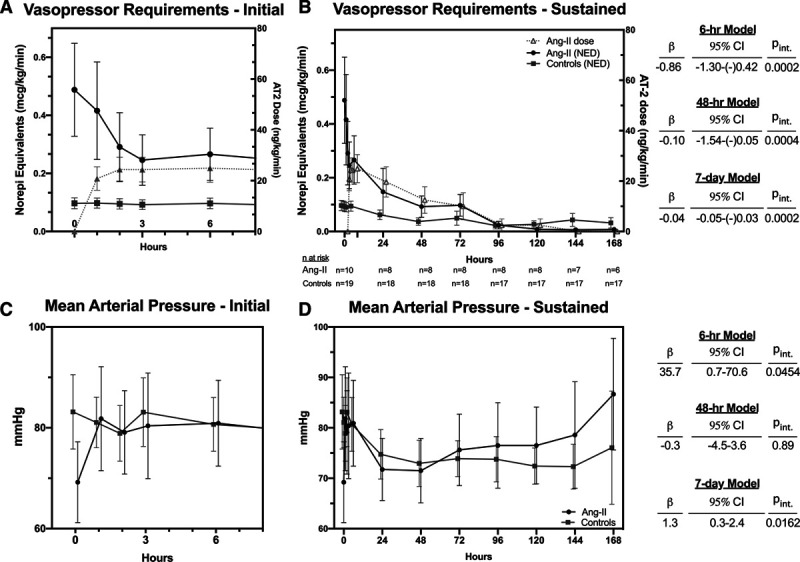
Main outcomes were trajectories of vasopressor requirements (in norepinephrine-equivalent dose) and mean arterial pressure. Additionally assessed trajectories were respiratory (Pao/Fio, Paco), metabolic (pH, creatinine), and coagulation (d-dimer) dysfunction indices after time-zero. We also recorded adverse events and clinical outcomes. Trajectories were analyzed using mixed-effects models for immediate (first 6 hr), early (48 hr), and sustained (7 d) responses. Twenty-nine patients ( = 10 treated, = 19 control) were identified. Despite matching, angiotensin-II-treated patients had markedly greater vasopressor requirements (mean: 0.489 vs 0.097 µg/kg/min), oxygenation impairment, and acidosis at time-zero. Nonetheless, angiotensin-II treatment was associated with an immediate and sustained reduction in norepinephrine-equivalent dose (6 hr model: β = -0.036 µg/kg/min/hr; 95% CI: -0.054 to -0.018 µg/kg/min/hr, =0.0002) (7 d model: β = -0.04 µg/kg/min/d, 95% CI: -0.05 to -0.03 µg/kg/min/d; = 0.0002). Compared with controls, angiotensin-II-treated patients had significantly faster improvement in mean arterial pressure, hypercapnia, acidosis, baseline-corrected creatinine, and d-dimer. Three thrombotic events occurred, all in control patients.
Angiotensin-II treatment for coronavirus disease 2019-induced distributive shock was associated with rapid improvement in multiple physiologic indices. Angiotensin-II in coronavirus disease 2019-induced shock warrants further study.
评估2019冠状病毒病所致呼吸衰竭和分布性休克患者对血管紧张素II治疗的早期生理反应。
回顾性连续样本队列研究。
2019冠状病毒病疫情期间纽约的三个医学重症监护病房。
所有患者因呼吸衰竭入住重症监护病房,并因分布性休克接受去甲肾上腺素治疗。
治疗组为接受血管紧张素II治疗≥1小时的患者。时间零点为开始使用血管紧张素II的时间。通过2:1分层匹配程序确定对照组,匹配因素包括:1)入院日期和科室;2)特定器官支持方式;3)年龄;4)慢性肺、心血管和肾脏疾病;5)性别。对照组的时间零点为开始使用血管升压药后21小时,即治疗组开始使用血管紧张素II前血管升压药治疗的平均持续时间。
主要结局指标为血管升压药需求量(以去甲肾上腺素等效剂量表示)和平均动脉压的变化轨迹。另外评估的变化轨迹指标为时间零点后的呼吸功能(动脉血氧分压/吸入氧分数值、动脉血二氧化碳分压)、代谢功能(pH值、肌酐)和凝血功能(D-二聚体)障碍指标。我们还记录了不良事件和临床结局。使用混合效应模型分析变化轨迹,以评估即刻(最初6小时)、早期(48小时)和持续(7天)反应。共纳入29例患者(治疗组10例,对照组19例)。尽管进行了匹配,但血管紧张素II治疗的患者在时间零点时血管升压药需求量明显更高(平均值:0.489 vs 0.097μg/kg/min),存在氧合障碍和酸中毒。尽管如此,血管紧张素II治疗与去甲肾上腺素等效剂量的即刻和持续降低相关(6小时模型:β=-0.036μg/kg/min/hr;95%CI:-0.054至-0.018μg/kg/min/hr,P=0.0002)(7天模型:β=-0.04μg/kg/min/d,95%CI:-0.05至-0.03μg/kg/min/d;P=0.0002)。与对照组相比,血管紧张素II治疗的患者平均动脉压、高碳酸血症、酸中毒、基线校正后的肌酐和D-二聚体的改善明显更快。发生了3例血栓形成事件,均在对照组患者中。
血管紧张素II治疗2019冠状病毒病所致分布性休克与多种生理指标的快速改善相关。血管紧张素II在2例19冠状病毒病所致休克中的应用值得进一步研究。