Non-Communicable Diseases Theme, Medical Research Council/Uganda Virus Research Institute and London School of Hygiene and Tropical Medicine (MRC/UVRI & LSHTM) Uganda Research Unit, Plot 51-59, Nakiwogo Road, P. O. BOX 49, Entebbe, Uganda.
Department of Endocrinology and Diabetes, Queen Mary University of London, Mile End Road, London, UK.
BMC Pregnancy Childbirth. 2020 Oct 19;20(1):635. doi: 10.1186/s12884-020-03325-9.
The diagnosis of hyperglycaemia in sub-Saharan Africa (SSA) is challenging. Blood glucose levels obtained during oral glucose tolerance test (OGTT) may not reflect home glycaemic profiles. We compare OGTT results with home glycaemic profiles obtained using the FreeStyle Libre continuous glucose monitoring device (FSL-CGM).
Twenty-eight women (20 with gestational diabetes [GDM], 8 controls) were recruited following OGTT between 24 and 28 weeks of gestation. All women wore the FSL-CGM device for 48-96 h at home in early third trimester, and recorded a meal diary. OGTT was repeated on the final day of FSL-CGM recording. OGTT results were compared with ambulatory glycaemic variables, and repeat OGTT was undertaken whilst wearing FSL-CGM to determine accuracy of the device.
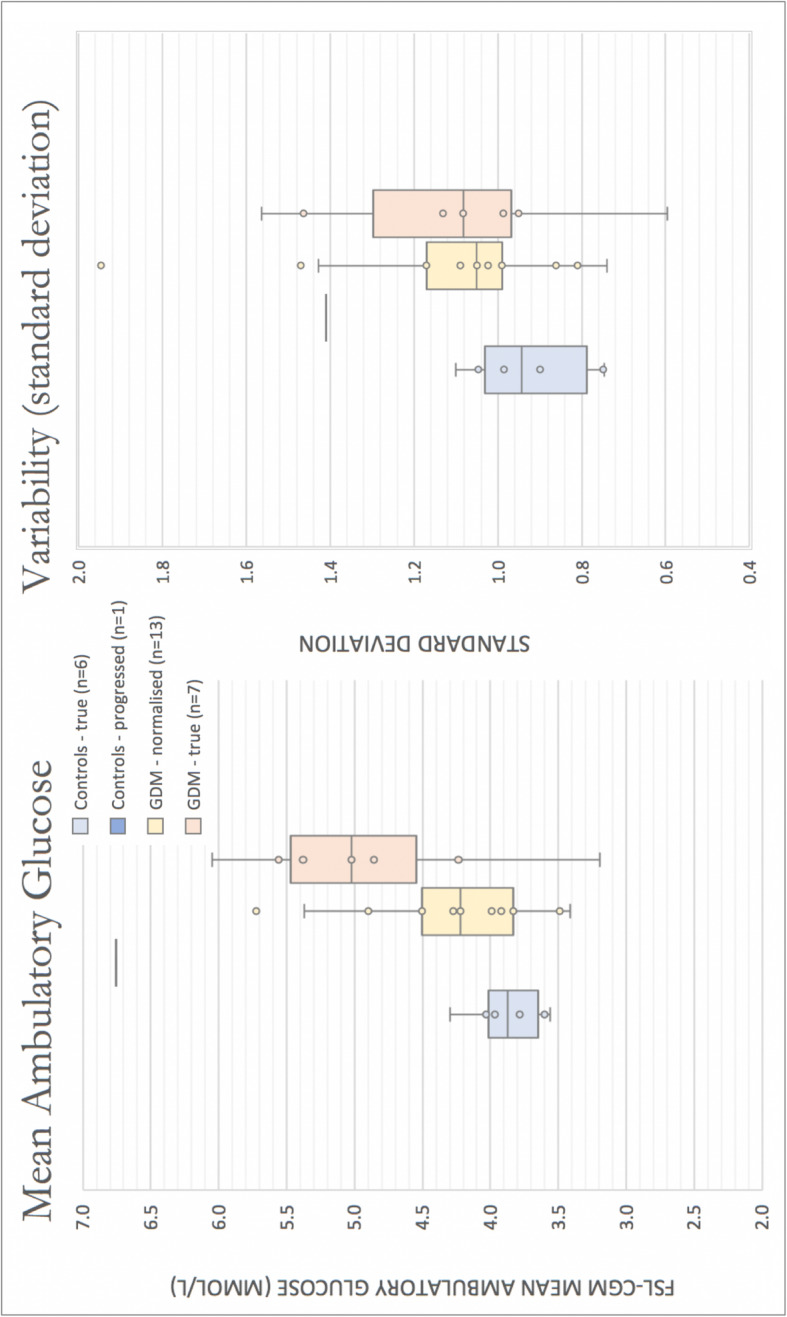
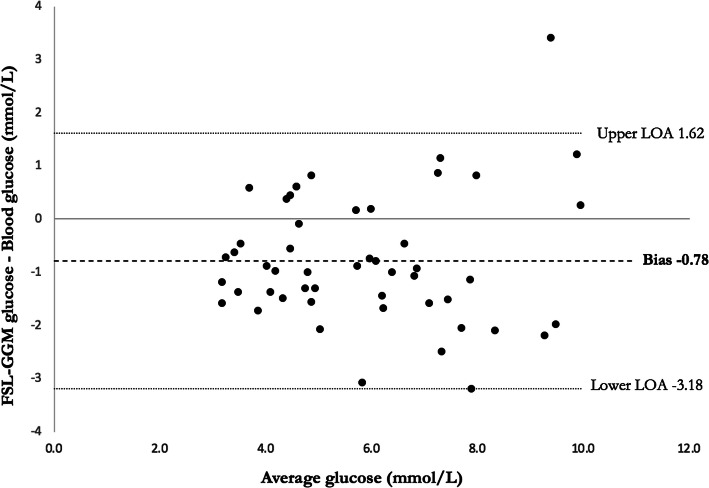
FSL-CGM results were available for 27/28 women with mean data capture 92.8%. There were significant differences in the ambulatory fasting, post-prandial peaks, and mean glucose between controls in whom both primary and secondary OGTT was normal (n = 6) and those with two abnormal OGTTs or "true" GDM (n = 7). There was no difference in ambulatory mean glucose between these controls and the 13 women who had an abnormal primary OGTT and normal repeat OGTT. These participants had significantly lower body mass index (BMI) than the true GDM group (29.0 Vs 36.3 kg/m, p-value 0.014). Paired OGTT/FSL-CGM readings revealed a Mean Absolute difference (MAD) -0.58 mmol/L and Mean Absolute Relative Difference (MARD) -11.9%. Bland-Altman plot suggests FSL-CGM underestimated blood glucose by approximately 0.78 mmol/L.
Diagnosis of GDM on a single OGTT identifies a proportion of women who do not have a significantly higher home glucose levels than controls. This raises questions about factors which may affect the reproducibility of OGTT in this population, including food insecurity and atypical phenotypes of diabetes. More investigation is needed to understand the suitability of the OGTT as a diagnostic test in sub-Saharan Africa.
在撒哈拉以南非洲(SSA),高血糖的诊断具有挑战性。口服葡萄糖耐量试验(OGTT)期间获得的血糖水平可能无法反映家庭血糖谱。我们将 OGTT 结果与使用 FreeStyle Libre 连续血糖监测仪(FSL-CGM)获得的家庭血糖谱进行比较。
在 24-28 孕周期间进行 OGTT 后,招募了 28 名女性(20 名患有妊娠期糖尿病[GDM],8 名对照)。所有女性在妊娠晚期的家中佩戴 FSL-CGM 设备 48-96 小时,并记录膳食日记。在 FSL-CGM 记录的最后一天重复 OGTT。将 OGTT 结果与动态血糖变量进行比较,并在佩戴 FSL-CGM 时进行重复 OGTT,以确定设备的准确性。
FSL-CGM 结果可用于 27/28 名女性,平均数据捕获率为 92.8%。在控制组中,OGTT 两次正常(n=6)和两次异常或“真正”GDM(n=7)的女性中,空腹、餐后峰值和平均血糖的动态有显著差异。在这些对照组和 13 名 OGTT 初次异常但重复 OGTT 正常的女性中,动态平均血糖无差异。这些参与者的体重指数(BMI)明显低于真正 GDM 组(29.0 对 36.3kg/m,p 值=0.014)。配对 OGTT/FSL-CGM 读数显示平均绝对差值(MAD)-0.58mmol/L 和平均绝对相对差值(MARD)-11.9%。Bland-Altman 图表明 FSL-CGM 低估了大约 0.78mmol/L 的血糖。
单次 OGTT 诊断 GDM 可识别出一部分女性的家庭血糖水平并不明显高于对照组。这引发了一些问题,即哪些因素可能影响 OGTT 在该人群中的可重复性,包括粮食不安全和糖尿病的非典型表型。需要进一步研究以了解 OGTT 作为撒哈拉以南非洲诊断试验的适用性。