School of Women's and Children's Health, University of New South Wales Sydney, Locked Bag 2000, Barker Street, Randwick, NSW 2031, Australia.
Diabetes Clinic, Royal Hospital for Women, Barker street-Randwick, NSW 2031, Australia.
J Diabetes Res. 2022 Oct 17;2022:5142918. doi: 10.1155/2022/5142918. eCollection 2022.
Gestational diabetes mellitus (GDM) is diabetes first diagnosed in pregnancy. GDM, together with its short- and long-term negative outcomes, is increasing in incidence all over the world. The current diagnostic method for GDM, the oral glucose tolerance test (OGTT), is dated and has been reported as inconvenient for women as well as poorly reproducible and reliable.
We aimed at assessing the acceptability, feasibility, and accuracy of continuous glucose monitoring (CGM) as a diagnostic test for GDM and explore its correlation with the OGTT and risk factors for GDM.
In this prospective cohort study, pregnant women due for or having completed OGTT underwent CGM for seven days, performing daily finger-prick blood glucose levels before completing an acceptability questionnaire. Data on GDM risk factors and CGM variability were analyzed and compared with OGTT results.
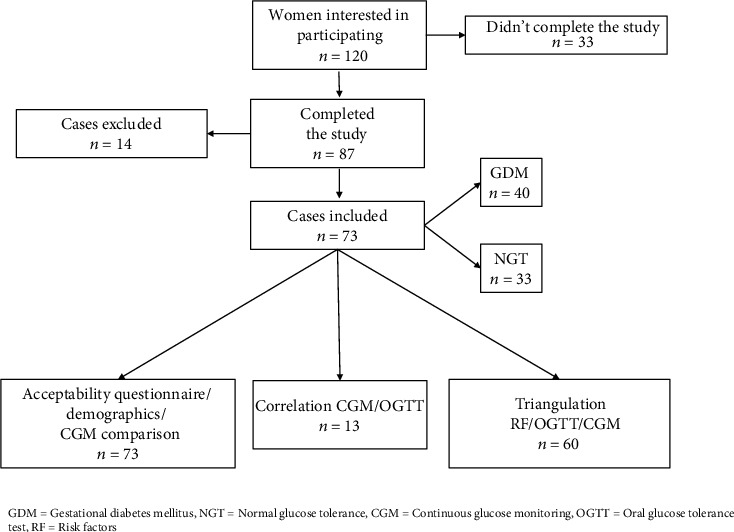
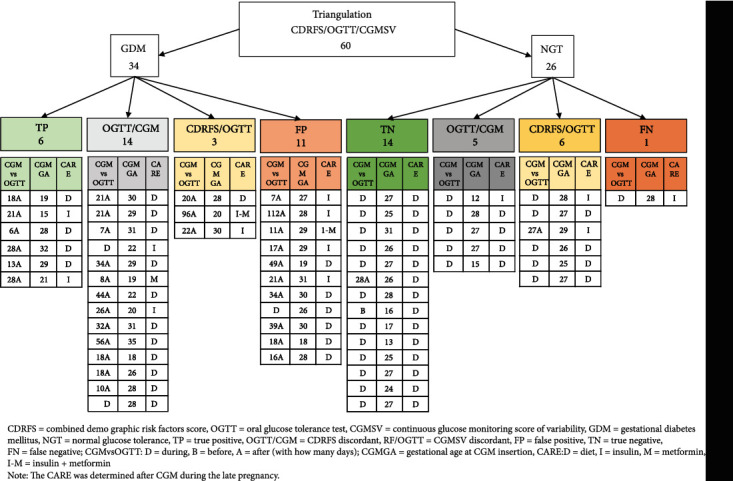
Seventy-three women completed CGM (40 GDM, 33 normal glucose tolerances); 34 concurrently underwent OGTT. CGM was acceptable and generally well-tolerated, with skin irritation/itchiness the only adverse event (11 mild, one severe). CGM and OGTT strongly correlated for fasting glucose values ( = 0.86, < 0.05) only. Triangulating GDM risk factors, OGTT results and CGM variability parameters with the application of machine learning highlighted the possibility of unmasking false positive (11 showed low CGM variability and demographic risks but positive OGTT) and false-negative OGTT diagnoses (1 showed high CGM variability and demographic risks but negative OGTT).
CGM was well-tolerated, showing poorer glycaemic control in GDM, and revealing potential misdiagnosis of the OGTT when combined with GDM risk factors. Future research is needed to determine cut-off values for CGM-defined and OGTT-independent screening criteria for GDM.
妊娠期糖尿病(GDM)是指在怀孕期间首次诊断出的糖尿病。GDM 及其短期和长期不良后果的发病率在全球范围内都在增加。目前 GDM 的诊断方法是口服葡萄糖耐量试验(OGTT),这种方法已经过时,据报道对女性来说既不方便,也不可靠。
我们旨在评估连续血糖监测(CGM)作为 GDM 诊断测试的可接受性、可行性和准确性,并探讨其与 OGTT 及 GDM 风险因素的相关性。
在这项前瞻性队列研究中,进行或已完成 OGTT 的孕妇接受了为期七天的 CGM 检查,在完成可接受性问卷之前每天进行指尖血糖检测。分析了 GDM 风险因素和 CGM 变异性的数据,并与 OGTT 结果进行了比较。
73 名女性完成了 CGM(40 名 GDM,33 名糖耐量正常);34 名女性同时进行了 OGTT。CGM 是可接受的,通常耐受性良好,只有皮肤刺激/瘙痒这一种不良事件(11 例轻度,1 例重度)。CGM 和 OGTT 仅在空腹血糖值方面具有强相关性( = 0.86, < 0.05)。通过应用机器学习对 GDM 风险因素、OGTT 结果和 CGM 变异性参数进行三角剖分,突出了掩盖 OGTT 假阳性(11 例显示低 CGM 变异性和人口统计学风险但 OGTT 阳性)和假阴性 OGTT 诊断(1 例显示高 CGM 变异性和人口统计学风险但 OGTT 阴性)的可能性。
CGM 耐受性良好,GDM 患者的血糖控制较差,并在结合 GDM 风险因素时揭示了 OGTT 潜在的误诊。需要进一步的研究来确定 CGM 定义和 OGTT 独立的 GDM 筛查标准的截断值。