Nuffield professor of primary care and head of department.
National Infection Service, Public Health England, London.
Br J Gen Pract. 2020 Nov 26;70(701):e890-e898. doi: 10.3399/bjgp20X713393. Print 2020 Dec.
The SARS-CoV-2 pandemic has passed its first peak in Europe.
To describe the mortality in England and its association with SARS-CoV-2 status and other demographic and risk factors.
Cross-sectional analyses of people with known SARS-CoV-2 status in the Oxford RCGP Research and Surveillance Centre (RSC) sentinel network.
Pseudonymised, coded clinical data were uploaded from volunteer general practice members of this nationally representative network ( = 4 413 734). All-cause mortality was compared with national rates for 2019, using a relative survival model, reporting relative hazard ratios (RHR), and 95% confidence intervals (CI). A multivariable adjusted odds ratios (OR) analysis was conducted for those with known SARS-CoV-2 status ( = 56 628, 1.3%) including multiple imputation and inverse probability analysis, and a complete cases sensitivity analysis.
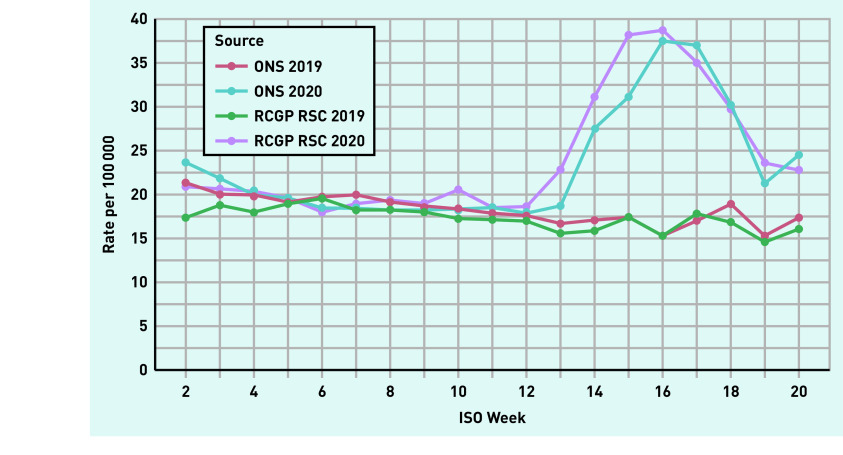
Mortality peaked in week 16. People living in households of ≥9 had a fivefold increase in relative mortality (RHR = 5.1, 95% CI = 4.87 to 5.31, <0.0001). The ORs of mortality were 8.9 (95% CI = 6.7 to 11.8, <0.0001) and 9.7 (95% CI = 7.1 to 13.2, <0.0001) for virologically and clinically diagnosed cases respectively, using people with negative tests as reference. The adjusted mortality for the virologically confirmed group was 18.1% (95% CI = 17.6 to 18.7). Male sex, population density, black ethnicity (compared to white), and people with long-term conditions, including learning disability (OR = 1.96, 95% CI = 1.22 to 3.18, = 0.0056) had higher odds of mortality.
The first SARS-CoV-2 peak in England has been associated with excess mortality. Planning for subsequent peaks needs to better manage risk in males, those of black ethnicity, older people, people with learning disabilities, and people who live in multi-occupancy dwellings.
SARS-CoV-2 大流行已在欧洲度过第一个高峰期。
描述英格兰的死亡率及其与 SARS-CoV-2 状态以及其他人口统计学和危险因素的关系。
对牛津 RCGP 研究和监测中心(RSC)监测网络中已知 SARS-CoV-2 状态的人群进行横断面分析。
从该具有全国代表性的网络中的志愿全科医生成员上传了匿名化、编码的临床数据(n = 4 413 734)。使用相对生存率模型比较了全因死亡率与 2019 年的全国死亡率,报告相对危险比(RHR)和 95%置信区间(CI)。对已知 SARS-CoV-2 状态者(n = 56 628,1.3%)进行了多变量调整后的比值比(OR)分析,包括多重插补和逆概率分析,以及完全病例敏感性分析。
死亡率在第 16 周达到峰值。居住在≥9 人的家庭中的人,其相对死亡率增加了五倍(RHR = 5.1,95%CI = 4.87 至 5.31,<0.0001)。使用阴性检测结果作为参考,与临床诊断病例相比,病毒学诊断病例的死亡率 OR 分别为 8.9(95%CI = 6.7 至 11.8,<0.0001)和 9.7(95%CI = 7.1 至 13.2,<0.0001)。经病毒学证实的病例的调整死亡率为 18.1%(95%CI = 17.6 至 18.7)。男性、人口密度、黑人种族(与白人相比)以及患有长期疾病(包括学习障碍)的人(OR = 1.96,95%CI = 1.22 至 3.18,P = 0.0056)的死亡率更高。
英格兰的第一个 SARS-CoV-2 高峰与超额死亡率相关。规划随后的高峰需要更好地管理男性、黑人种族、老年人、学习障碍患者以及居住在多住户住宅中的人的风险。