Nuffield Department of Primary Care Health Sciences, University of Oxford, Radcliffe Observatory Quarter, Woodstock Road, Oxford OX2 6GG, UK.
Public Health England, London NW9 5EQ, UK.
J Infect. 2020 Nov;81(5):785-792. doi: 10.1016/j.jinf.2020.08.037. Epub 2020 Aug 25.
Few studies report contributors to the excess mortality in England during the first wave of coronavirus disease 2019 (COVID-19) infection. We report the absolute excess risk (AER) of mortality and excess mortality rate (EMR) from a nationally representative COVID-19 sentinel surveillance network including known COVID-19 risk factors in people aged 45 years and above.
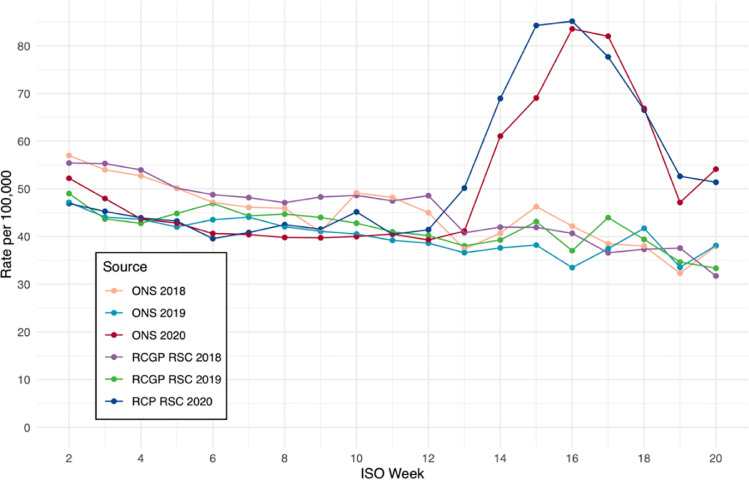
Pseudonymised, coded clinical data were uploaded from contributing primary care providers (N = 1,970,314, ≥45years). We calculated the AER in mortality by comparing mortality for weeks 2 to 20 this year with mortality data from the Office for National Statistics (ONS) from 2018 for the same weeks. We conducted univariate and multivariate analysis including preselected variables. We report AER and EMR, with 95% confidence intervals (95% CI).
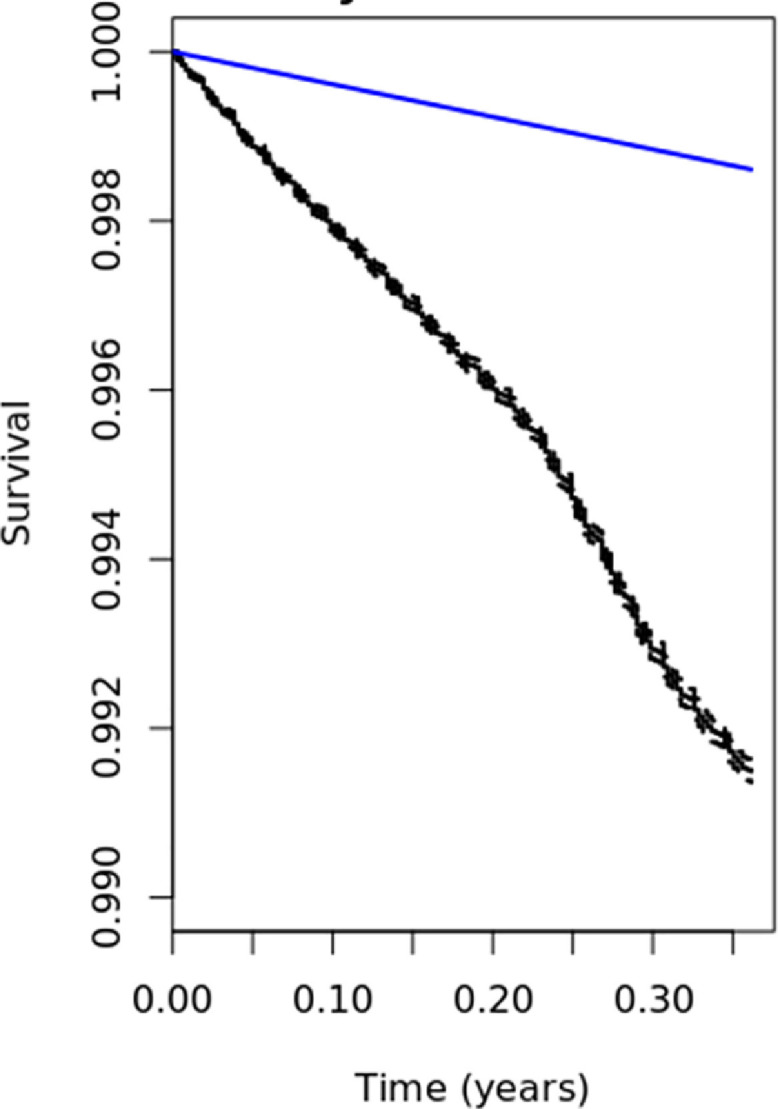
The AER of mortality was 197.8/10,000 person years (95%CI:194.30-201.40). The EMR for male gender, compared with female, was 1.4 (95%CI:1.35-1.44, p<0.00); for our oldest age band (≥75 years) 10.09 (95%CI:9.46-10.75, p<0.00) compared to 45-64 year olds; Black ethnicity's EMR was 1.17 (95%CI: 1.03-1.33, p<0.02), reference white; and for dwellings with ≥9 occupants 8.01 (95%CI: 9.46-10.75, p<0.00). Presence of all included comorbidities significantly increased EMR. Ranked from lowest to highest these were: hypertension, chronic kidney disease, chronic respiratory and heart disease, and cancer or immunocompromised.
The absolute excess mortality was approximately 2 deaths per 100 person years in the first wave of COVID-19. More personalised shielding advice for any second wave should include ethnicity, comorbidity and household size as predictors of risk.
很少有研究报告导致英格兰在 2019 年冠状病毒病(COVID-19)感染第一波期间死亡率过高的因素。我们报告了包括年龄在 45 岁及以上人群中已知 COVID-19 危险因素在内的全国性 COVID-19 监测网络的绝对超额死亡率(AER)和超额死亡率(EMR)。
从参与的初级保健提供者(N=1,970,314 人,年龄≥45 岁)上传匿名编码的临床数据。我们通过将今年第 2 周至第 20 周的死亡率与同期国家统计局(ONS)的死亡率数据进行比较,计算出死亡率的 AER。我们进行了单变量和多变量分析,包括预先选择的变量。我们报告 AER 和 EMR,并提供 95%置信区间(95%CI)。
死亡率的 AER 为 197.8/10000 人年(95%CI:194.30-201.40)。与女性相比,男性的 EMR 为 1.4(95%CI:1.35-1.44,p<0.00);对于我们最年长的年龄组(≥75 岁)为 10.09(95%CI:9.46-10.75,p<0.00),与 45-64 岁相比;黑人的 EMR 为 1.17(95%CI:1.03-1.33,p<0.02),参考白人;居住人数≥9 人的 EMR 为 8.01(95%CI:9.46-10.75,p<0.00)。存在所有包括的合并症都会显著增加 EMR。从最低到最高,这些疾病依次为:高血压、慢性肾脏病、慢性呼吸和心脏病以及癌症或免疫功能低下。
在 COVID-19 感染的第一波中,绝对超额死亡率约为每 100 人年 2 人死亡。如果出现第二波疫情,任何个性化的防护建议都应将种族、合并症和家庭规模作为风险预测因素。