Park Jun-Ook, Park Young Min, Jeong Woo-Jin, Shin Yoo Seob, Hong Yong Tae, Choi Ik Joon, Kim Ji Won, Woo Seung Hoon, Kim Yeon Soo, Chang Jae Won, Kim Min-Sik, Jung Kwang-Yoon, Ahn Soon-Hyun, Kim Chul-Ho, Hong Ki Hwan, Chung Phil-Sang, Kim Young-Mo, Kim Se-Heon, Baek Seung-Kuk
Department of Otolaryngology-Head and Neck Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Department of Otorhinolaryngology-Head and Neck Surgery, Yonsei University College of Medicine, Seoul, Korea.
Clin Exp Otorhinolaryngol. 2021 May;14(2):225-234. doi: 10.21053/ceo.2020.01732. Epub 2020 Sep 25.
Head and neck squamous cell carcinomas (HNSCs) are frequently diagnosed at the locoregional advanced stage (stage IVa), but controversy remains regarding whether stage IVa HSNCs should be treated with upfront surgery or definitive chemoradiation therapy (CRT). The purpose of this study was to compare overall survival (OS) and disease-free survival (DFS) in patients with stage IVa HNSC treated primarily by surgery with curative intent with/without (neo)adjuvant treatment (surgery group) versus those treated primarily with CRT (CRT group).
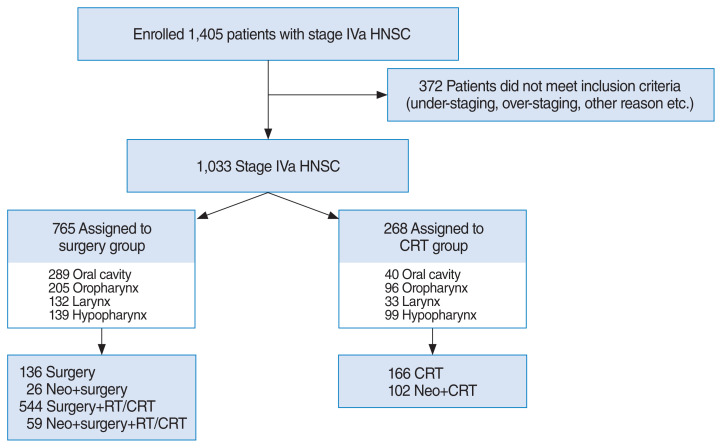
We reviewed data of 1,033 patients with stage IVa HNSC treated with curative intent at 17 cancer centers between 2010 and 2016.
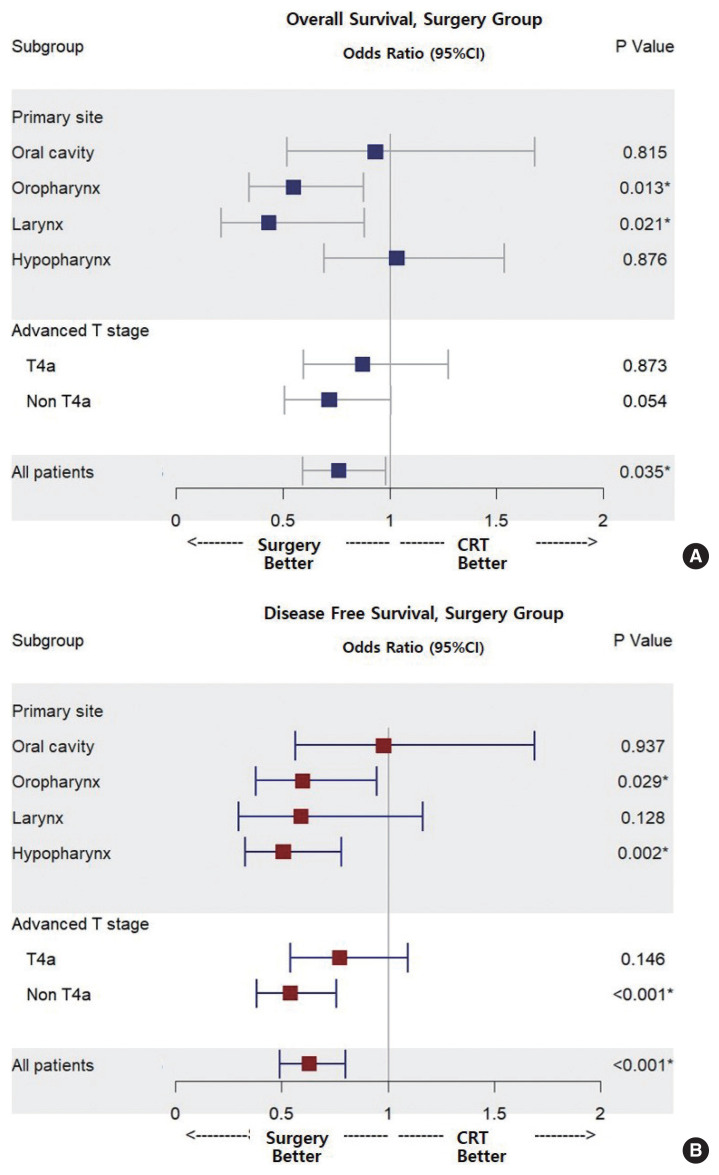
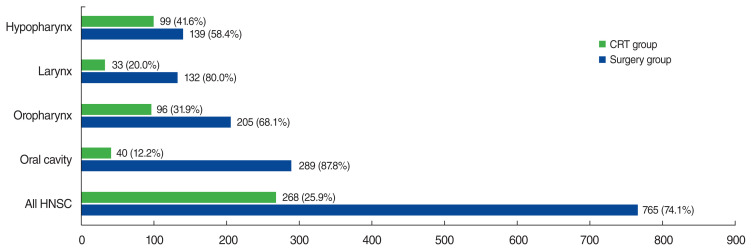
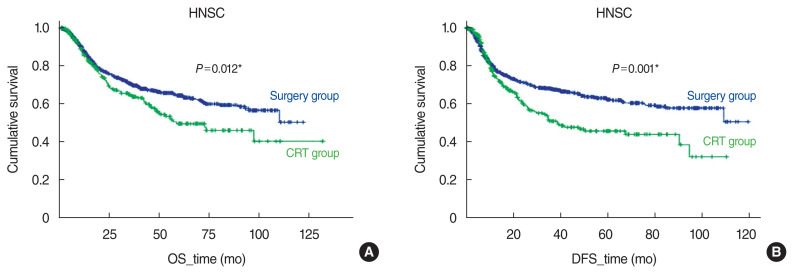
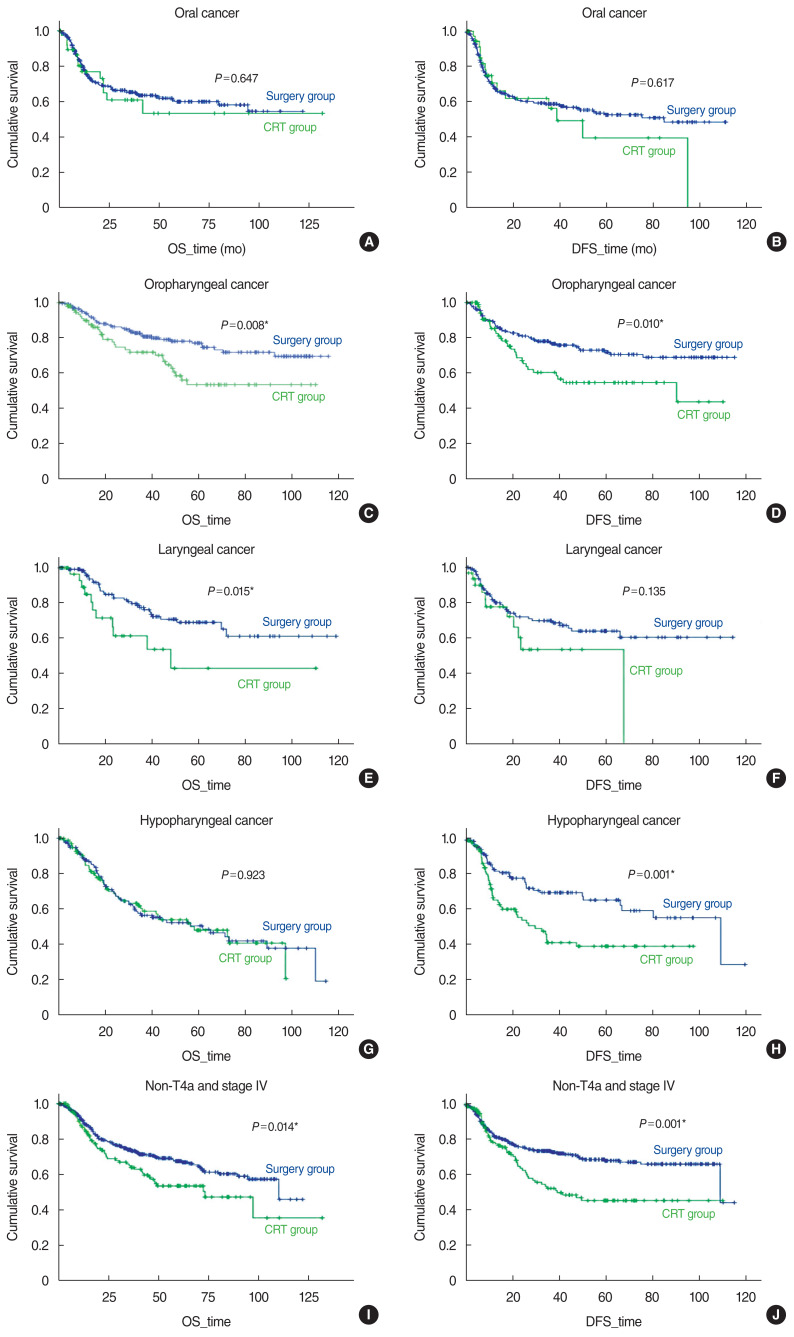
Among 1,033 patients, 765 (74.1%) received upfront surgery and 268 (25.9%) received CRT. The 5-year OS and DFS rates were 64.4% and 62.0% in the surgery group and 49.5% and 45.4% in the CRT group, respectively. In multivariate analyses, OS and DFS were better in the surgery group than in the CRT group (odds ratio [OR] for death, 0.762; 95% confidence interval [CI], 0.592-0.981; OR for recurrence, 0.628; 95% CI, 0.492-0.802). In subgroup analyses, the OS and DFS of patients with oropharyngeal cancer were better in the surgery group (OR for death, 0.548; 95% CI, 0.341-0.879; OR for recurrence, 0.598; 95% CI, 0.377-0.948). In the surgery group, patients with laryngeal cancer showed better OS (OR for death, 0.432; 95% CI, 0.211-0.882), while those with hypopharyngeal cancer DFS was improved (OR for recurrence, 0.506; 95% CI, 0.328-0.780).
A survival benefit from surgery may be achieved even in patients with stage IVa HNSC, particularly those with oropharyngeal and laryngeal cancer. Surgery led to a reduction in the recurrence rate in patients with hypopharyngeal cancer.
头颈部鳞状细胞癌(HNSCs)常在局部晚期(IVa期)被诊断出来,但对于IVa期HNSCs应接受 upfront 手术还是确定性放化疗(CRT)仍存在争议。本研究的目的是比较主要接受根治性手术并伴有或不伴有(新)辅助治疗的IVa期HNSC患者(手术组)与主要接受CRT的患者(CRT组)的总生存期(OS)和无病生存期(DFS)。
我们回顾了2010年至2016年间17个癌症中心1033例接受根治性治疗的IVa期HNSC患者的数据。
在1033例患者中,765例(74.1%)接受了 upfront 手术,268例(25.9%)接受了CRT。手术组的5年OS率和DFS率分别为64.4%和62.0%,CRT组分别为49.5%和45.4%。在多变量分析中,手术组的OS和DFS优于CRT组(死亡比值比[OR],0.762;95%置信区间[CI],0.592 - 0.981;复发OR,0.628;95%CI,0.492 - 0.802)。在亚组分析中,口咽癌患者的手术组OS和DFS更好(死亡OR,0.548;95%CI,0.341 - 0.879;复发OR,0.598;95%CI,0.377 - 0.948)。在手术组中,喉癌患者的OS更好(死亡OR,0.432;95%CI,0.211 - 0.882),而下咽癌患者的DFS有所改善(复发OR,0.506;95%CI,0.328 - 0.780)。
即使是IVa期HNSC患者,尤其是口咽癌和喉癌患者,手术也可能带来生存获益。手术降低了下咽癌患者的复发率。