Taenzer Andreas H, Patel Shilpa J, Allen Todd L, Doerfler Martin E, Park Tae-Ryong, Savitz Lucy A, Park John G
Department of Anesthesiology, Dartmouth Hitchcock Medical Center, Lebanon, NH.
Department of Pediatrics, University of Hawaii John A. Burns School of Medicine, Honolulu, HI.
Mayo Clin Proc Innov Qual Outcomes. 2020 Aug 19;4(5):537-541. doi: 10.1016/j.mayocpiqo.2020.05.008. eCollection 2020 Oct.
To determine whether rapid administration of a crystalloid bolus of 30 mL/kg within 3 hours of presentation harms or benefits hypotensive patients with sepsis with a history of congestive heart failure (CHF).
A retrospective cohort study using Medicare claims data enhanced by medical record data from members of the High Value Healthcare Collaborative from July 1, 2013, to June 30, 2015, examining patients with a history of CHF who did (fluid bundle compliant [FBC]) or did not (NFBC) receive a volume bolus of 30 mL/kg within 3 hours of presentation to the emergency department. A proportional Cox hazard model was used to evaluate the association of FBC with 1-year survival.
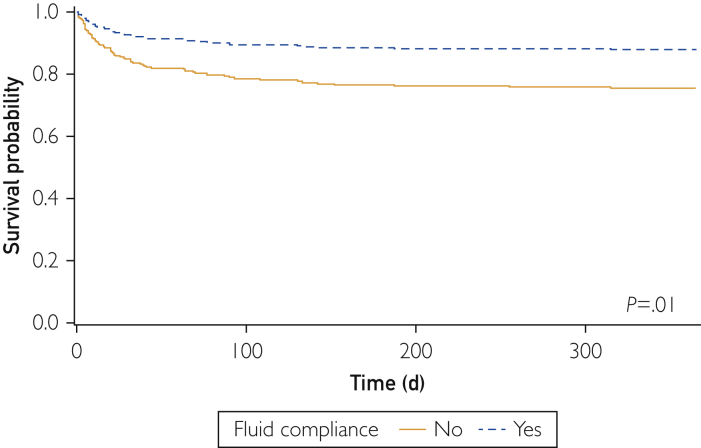
Of the 211 patients examined, 190 were FBC and 21 were NFBC. The FBC patients had higher average hierarchical condition category scores but were otherwise similar to NFBC patients. The NFBC patients had higher adjusted in-hospital and postdischarge mortality rates. The risk-adjusted 1-year mortality rate was higher for NFBC patients (hazard ratio, 2.18; 95% CI, 1.2 to 4.0; =.01) than for FBC patients.
In a retrospective claim data-based study of elderly patients with a history of CHF presenting with severe sepsis or septic shock, there is an association of improved mortality with adherence to the initial fluid resuscitation guidelines as part of the 3-hour sepsis bundle.
确定在就诊3小时内快速给予30 mL/kg晶体液推注对有充血性心力衰竭(CHF)病史的脓毒症低血压患者是有害还是有益。
一项回顾性队列研究,使用2013年7月1日至2015年6月30日期间高价值医疗协作组织成员的医保理赔数据并辅以病历数据,研究有CHF病史的患者,这些患者在急诊科就诊3小时内接受(符合液体推注组 [FBC])或未接受(非FBC组 [NFBC])30 mL/kg的容量推注。采用比例风险Cox模型评估FBC与1年生存率的关联。
在211例接受检查的患者中,190例为FBC组,21例为NFBC组。FBC组患者的平均分层病情类别得分较高,但在其他方面与NFBC组患者相似。NFBC组患者的住院调整死亡率和出院后死亡率较高。NFBC组患者的风险调整1年死亡率高于FBC组患者(风险比,2.18;95%置信区间,1.2至4.0;P =.01)。
在一项基于回顾性理赔数据的研究中,对于有CHF病史且出现严重脓毒症或脓毒性休克的老年患者,作为3小时脓毒症集束治疗一部分的初始液体复苏指南的依从性与死亡率改善相关。