Jones Timothy W, Chase Aaron M, Bruning Rebecca, Nimmanonda Naphun, Smith Susan E, Sikora Andrea
Department of Clinical and Administrative Pharmacy, University of Georgia College of Pharmacy, Augusta, GA, USA.
Department of Pharmacy, Augusta University Medical Center, Augusta, GA, USA.
Clin Med Insights Cardiol. 2022 May 13;16:11795468221095875. doi: 10.1177/11795468221095875. eCollection 2022.
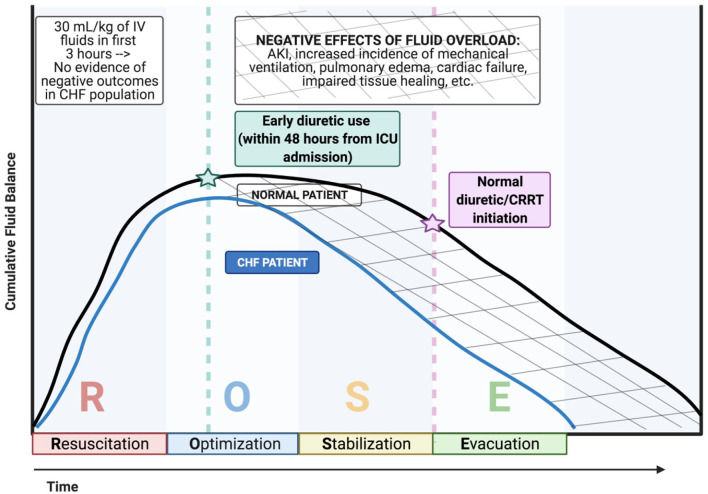
De-resuscitation practices in septic patients with heart failure (HF) are not well characterized. This study aimed to determine if diuretic initiation within 48 hours of intensive care unit (ICU) admission was associated with a positive fluid balance and patient outcomes.
This single-center, retrospective cohort study included adult patients with an established diagnosis of HF admitted to the ICU with sepsis or septic shock. The primary outcome was the incidence of positive fluid balance in patients receiving early (<48 hours) versus late (>48 hours) initiation of diuresis. Secondary outcomes included hospital mortality, ventilator-free days, and hospital and ICU length of stay. Continuous variables were assessed using independent t-test or Mann-Whitney U, while categorical variables were evaluated using the Pearson Chi-squared test.
A total of 101 patients were included. Positive fluid balance was significantly reduced at 72 hours (-139 mL vs 4370 mL, < .001). The duration of mechanical ventilation (4 vs 5 days, = .129), ventilator-free days (22 vs 18.5 days, = .129), and in-hospital mortality (28 (38%) vs 12 (43%), = .821) were similar between groups. In a subgroup analysis excluding patients not receiving renal replacement therap (RRT) (n = 76), early diuretics was associated with lower incidence of mechanical ventilation (41 [73.2%] vs 20 (100%), = .01) and reduced duration of mechanical ventilation (4 vs 8 days, = .018).
Diuretic use within 48 hours of ICU admission in septic patients with HF resulted in less incidence of positive fluid balance. Early diuresis in this unique patient population warrants further investigation.
心力衰竭(HF)合并脓毒症患者的撤机实践尚无充分描述。本研究旨在确定重症监护病房(ICU)入院48小时内开始使用利尿剂是否与液体正平衡及患者预后相关。
本单中心回顾性队列研究纳入确诊为HF且因脓毒症或脓毒性休克入住ICU的成年患者。主要结局是早期(<48小时)与晚期(>48小时)开始利尿的患者中液体正平衡的发生率。次要结局包括医院死亡率、无呼吸机天数以及住院和ICU住院时间。连续变量采用独立t检验或Mann-Whitney U检验进行评估,分类变量采用Pearson卡方检验进行评估。
共纳入101例患者。72小时时液体正平衡显著降低(-139 mL对4370 mL,P<0.001)。两组间机械通气时间(4天对5天,P=0.129)、无呼吸机天数(22天对18.5天,P=0.129)和住院死亡率(28例[38%]对12例[43%],P=0.821)相似。在排除未接受肾脏替代治疗(RRT)的患者(n=76)的亚组分析中,早期使用利尿剂与机械通气发生率较低(41例[73.2%]对20例[100%],P=0.01)和机械通气时间缩短(4天对8天,P=0.018)相关。
HF合并脓毒症患者在ICU入院48小时内使用利尿剂可降低液体正平衡的发生率。在这一特殊患者群体中早期利尿值得进一步研究。