Centre de Pneumologie, Institut Universitaire de Cardiologie et de Pneumologie de Québec, Université Laval, Québec, QC, Canada.
GSK, Brentford, Middlesex, UK.
Respir Res. 2020 Oct 22;21(1):280. doi: 10.1186/s12931-020-01451-8.
Short-acting β-agonist (SABA) bronchodilators help alleviate symptoms in chronic obstructive pulmonary disease (COPD) and may be a useful marker of symptom severity. This analysis investigated whether SABA use impacts treatment differences between maintenance dual- and mono-bronchodilators in patients with COPD.
The Early MAXimisation of bronchodilation for improving COPD stability (EMAX) trial randomised symptomatic patients with low exacerbation risk not receiving inhaled corticosteroids 1:1:1 to once-daily umeclidinium/vilanterol 62.5/25 μg, once-daily umeclidinium 62.5 μg or twice-daily salmeterol 50 μg for 24 weeks. Pre-specified subgroup analyses stratified patients by median baseline SABA use (low, < 1.5 puffs/day; high, ≥1.5 puffs/day) to examine change from baseline in trough forced expiratory volume in 1 s (FEV), change in symptoms (Transition Dyspnoea Index [TDI], Evaluating Respiratory Symptoms-COPD [E-RS]), daily SABA use and exacerbation risk. A post hoc analysis used fractional polynomial modelling with continuous transformations of baseline SABA use covariates.
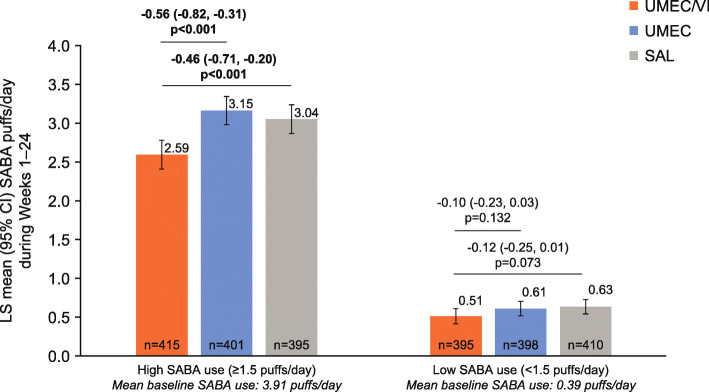
At baseline, patients in the high SABA use subgroup (mean: 3.91 puffs/day, n = 1212) had more severe airflow limitation, were more symptomatic and had worse health status versus patients in the low SABA use subgroup (0.39 puffs/day, n = 1206). Patients treated with umeclidinium/vilanterol versus umeclidinium demonstrated statistically significant improvements in trough FEV at Week 24 in both SABA subgroups (59-74 mL; p < 0.001); however, only low SABA users demonstrated significant improvements in TDI (high: 0.27 [p = 0.241]; low: 0.49 [p = 0.025]) and E-RS (high: 0.48 [p = 0.138]; low: 0.60 [p = 0.034]) scores. By contrast, significant reductions in mean SABA puffs/day with umeclidinium/vilanterol versus umeclidinium were observed only in high SABA users (high: - 0.56 [p < 0.001]; low: - 0.10 [p = 0.132]). Similar findings were observed when comparing umeclidinium/vilanterol and salmeterol. Fractional polynomial modelling showed baseline SABA use ≥4 puffs/day resulted in smaller incremental symptom improvements with umeclidinium/vilanterol versus umeclidinium compared with baseline SABA use < 4 puffs/day.
In high SABA users, there may be a smaller difference in treatment response between dual- and mono-bronchodilator therapy; the reasons for this require further investigation. SABA use may be a confounding factor in bronchodilator trials and in high SABA users; changes in SABA use may be considered a robust symptom outcome.
GlaxoSmithKline (study number 201749 [NCT03034915]).
短效β-激动剂(SABA)支气管扩张剂有助于缓解慢性阻塞性肺疾病(COPD)的症状,并且可能是症状严重程度的有用标志物。本分析研究了 COPD 患者中 SABA 使用是否会影响维持双支气管扩张剂和单支气管扩张剂治疗之间的差异。
早期最大程度地改善 COPD 稳定性的支气管扩张(EMAX)试验将低风险加重的症状性患者随机分为 1:1:1 组,分别接受每日一次乌美溴铵/维兰特罗 62.5/25μg、每日一次乌美溴铵 62.5μg 或每日两次沙美特罗 50μg 治疗,持续 24 周。根据中位基线 SABA 使用情况(低,<1.5 吸/天;高,≥1.5 吸/天)进行预先指定的亚组分析,以检查从基线到 trough 用力呼气量 1 秒(FEV)的变化、症状变化(过渡性呼吸困难指数[TDI]、评估呼吸症状-COPD[E-RS])、每日 SABA 使用和加重风险。事后分析使用分数多项式模型对基线 SABA 使用协变量进行连续变换。
在基线时,高 SABA 使用亚组(平均:3.91 吸/天,n=1212)的患者气流受限程度更严重,症状更严重,健康状况更差,而低 SABA 使用亚组(0.39 吸/天,n=1206)。与乌美溴铵相比,乌美溴铵/维兰特罗治疗的患者在第 24 周时 trough FEV 有统计学显著改善(59-74mL;p<0.001);然而,只有低 SABA 使用患者的 TDI(高:0.27[p=0.241];低:0.49[p=0.025])和 E-RS(高:0.48[p=0.138];低:0.60[p=0.034])评分有显著改善。相比之下,与乌美溴铵相比,乌美溴铵/维兰特罗仅在高 SABA 使用患者中观察到平均 SABA 用量/天的显著减少(高:-0.56[p<0.001];低:-0.10[p=0.132])。与沙美特罗相比,也观察到了类似的发现。分数多项式模型显示,基线 SABA 使用量≥4 吸/天与基线 SABA 使用量<4 吸/天相比,乌美溴铵/维兰特罗与乌美溴铵相比,症状改善的增量较小。
在高 SABA 使用患者中,双支气管扩张剂和单支气管扩张剂治疗之间的治疗反应可能存在较小的差异;这方面的原因需要进一步研究。SABA 使用可能是支气管扩张剂试验中的一个混杂因素,在高 SABA 使用患者中也是如此;SABA 使用的变化可以被认为是一个可靠的症状结果。
葛兰素史克(研究编号 201749[NCT03034915])。