Department of Morphology, Surgery and Experimental Medicine, Intensive Care Unit, Azienda Ospedaliera Universitaria Sant'Anna Hospital, Ferrara, Italy.
Department of Anesthesia, Critical Care and Emergency, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Via F. Sforza 35, 20122, Milan, Italy.
Crit Care. 2020 Oct 22;24(1):622. doi: 10.1186/s13054-020-03335-1.
The physiological behavior of lungs affected by the acute respiratory distress syndrome (ARDS) differs between inspiration and expiration and presents heterogeneous gravity-dependent distribution. This phenomenon, highlighted by the different distribution of opening/closing pressure and by the hysteresis of the pressure-volume curve, can be studied by CT scan, but the technique expose the patient to radiations, cannot track changes during time and is not feasible at the bedside. Electrical impedance tomography (EIT) could help in assessing at the bedside regional inspiratory and expiratory mechanical properties. We evaluated regional opening/closing pressures, hysteresis and atelectrauma during inspiratory and expiratory low-flow pressure-volume curves in ARDS using electrical impedance tomography.
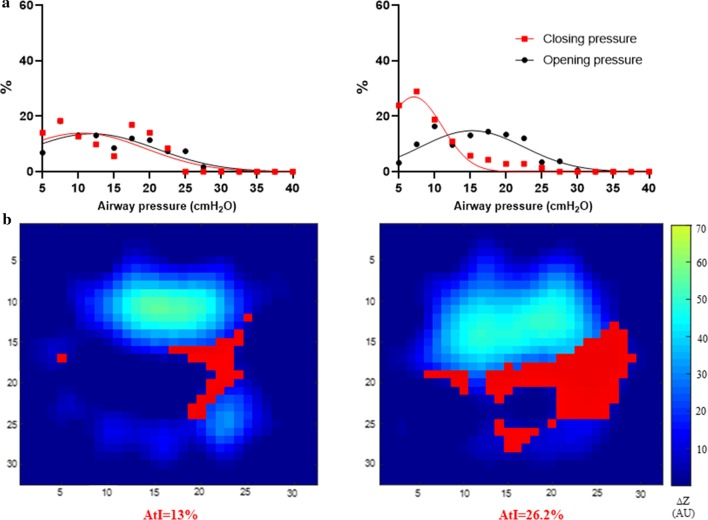
Pixel-level inspiratory and expiratory PV curves (PV) between 5 and 40 cmHO were constructed integrating EIT images and airway opening pressure signal from 8 ARDS patients. The lower inflection point in the inspiratory and expiratory PV were used to find opening (OP) and closing (CP) pressures. A novel atelectrauma index (AtI) was calculated as the percentage of pixels opening during the inspiratory and closing during the expiratory PV curves. The maximal hysteresis (HysMax) was calculated as the maximal difference between normalized expiratory and inspiratory PV curves. Analyses were conducted in the global, dependent and non-dependent lung regions.
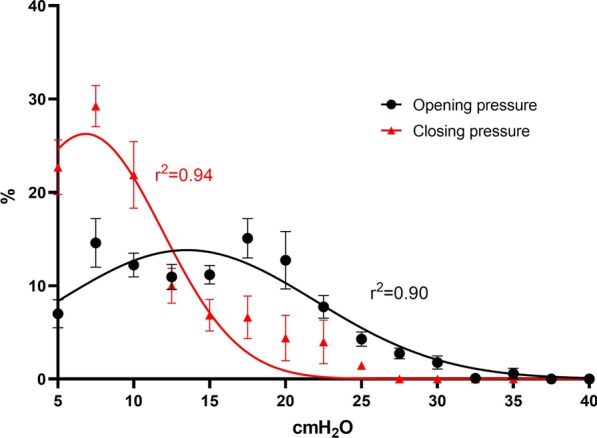
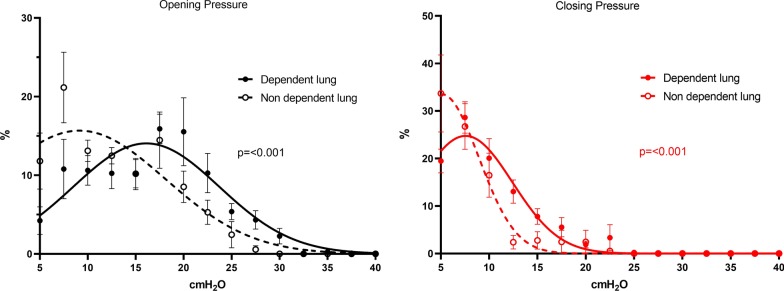
Gaussian distribution was confirmed for both global OP (r = 0.90) and global CP (r = 0.94). The two distributions were significantly different with higher values for OP (p < 0.0001). Regional OP and CP distributions were Gaussian, and in the dependent lung regions, both were significantly higher than in the non-dependent ones (p < 0.001). Both AtI and the HysMax were significantly higher in the dependent regions compared to the non-dependent ones (p < 0.05 for both).
Gravity impacts the regional distribution of opening and closing pressure, hysteresis and atelectrauma, with higher values in the dorsal lung. Regional differences between inspiratory and expiratory lung physiology are detectable at the bedside using EIT and could allow in-depth characterization of ARDS phenotypes and guide personalized ventilation settings.
急性呼吸窘迫综合征(ARDS)肺部的生理行为在吸气和呼气时不同,并呈现出异质性的重力依赖性分布。这种现象由开闭压的不同分布和压力-容积曲线的滞后性突出显示,可以通过 CT 扫描进行研究,但该技术会使患者暴露在辐射下,无法跟踪时间上的变化,并且在床边不可行。电阻抗断层成像(EIT)可以帮助在床边评估吸气和呼气时的区域性机械性能。我们使用电阻抗断层成像来评估 ARDS 患者在吸气和呼气低流量压力-容积曲线时的区域性开闭压、滞后性和肺泡萎陷伤。
从 8 名 ARDS 患者的 EIT 图像和气道开放压力信号中构建了 5 至 40 cmHO 之间的像素级吸气和呼气 PV 曲线(PV)。吸气和呼气 PV 的下拐点用于找到开口(OP)和关闭(CP)压力。计算了一种新的肺泡萎陷伤指数(AtI),作为吸气时开放的像素百分比和呼气时关闭的像素百分比。最大滞后(HysMax)作为归一化的呼气和吸气 PV 曲线之间的最大差异来计算。分析在整体、依赖和非依赖肺区进行。
全球 OP(r=0.90)和全球 CP(r=0.94)均呈高斯分布。两种分布有显著差异,OP 值较高(p<0.0001)。区域性 OP 和 CP 分布呈高斯分布,在依赖区,两者均显著高于非依赖区(p<0.001)。与非依赖区相比,依赖区的 AtI 和 HysMax 均显著升高(p<0.05)。
重力会影响开闭压、滞后性和肺泡萎陷伤的区域性分布,背部肺区的数值较高。EIT 可在床边检测到吸气和呼气时肺生理学的区域差异,并可深入表征 ARDS 表型并指导个性化通气设置。