Department of Clinical Epidemiology, Leibniz Institute for Prevention Research and Epidemiology-BIPS, Achterstraße 30, 28359, Bremen, Germany.
Department of Translational Medicine, University of Eastern Piedmont, Via Solaroli 17, 28100, Novara, Italy.
Drugs Aging. 2020 Dec;37(12):885-897. doi: 10.1007/s40266-020-00806-6. Epub 2020 Oct 23.
Medications with anticholinergic activity (MACs) are used to treat diseases common in older adults. Evidence on the association between anticholinergic burden (AB) and increased risk of fractures and osteoporosis or reduced bone mineral density (BMD) is inconsistent. Our aim was to conduct a systematic review of observational studies on AB with fractures and osteoporosis or reduced BMD and provide methodological appraisal of included studies.
We searched MEDLINE, EMBASE, Science Citation Index and CENTRAL as well as grey literature from database inception up to August 2020. Eligibility criteria were: observational design, AB-exposure measured through a scale, fracture of any type or osteoporosis or reduced BMD as outcome, and reported measure of association between exposure and outcome. No restrictions related to time, language or type of data were applied. Eligibility and risk of bias assessment as well as data extraction were performed independently by two reviewers. Risk of bias of the included studies was assessed using the Newcastle-Ottawa Scale and the RTI Item Bank.
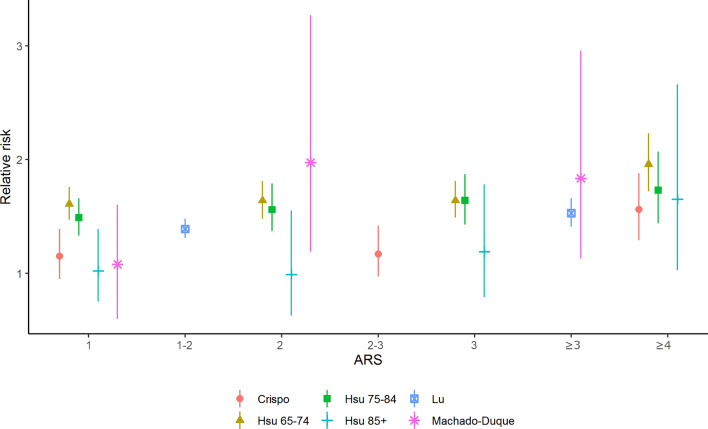
The majority of the nine included studies had low risk of bias but heterogeneous methodology. No study used a new user design. Seven studies reported an increased risk of fractures associated with AB. In four studies using the Anticholinergic Risk Scale (ARS), adjusted risk of fractures was increased by 2-61% for ARS = 1, by 0-97% for ARS = 2, by 19-84% for ARS = 3, and by 56-96% for ARS ≥ 4; in three studies the ARS was aggregated, risk increased by 39% for ARS = 1-2 and 17% for ARS = 2-3. Two studies reported increased risk of fractures of 14 and 52% in the highest AB-category and one study reported that change in ARS of ≥ 3 during hospitalization was associated with a 321% increased risk in fractures. Two studies did not find an association between AB and fractures. The association between AB and osteoporosis or reduced BMD could only be assessed in two studies, one reporting increased risk of lower BMD at Ward's triangle, the other reporting no association between AB and BMD T-score change at the femoral neck.
Our study suggests an association between AB and increased risk of fractures with possible dose-exposure gradient in studies using the ARS. The low number of studies and heterogeneity of methods calls for the conduct of more studies. We conducted a study investigating the risk of fractures associated with anticholinergic burden, which is the result of taking one or more medication with anticholinergic activity. The results of our study suggest that persons who experience anticholinergic burden might have a higher risk of fractures. However, since we were only able to include nine studies, more studies conducted in a similar way are needed.

具有抗胆碱能活性(MAC)的药物用于治疗老年人常见的疾病。关于抗胆碱能负担(AB)与骨折和骨质疏松症或骨密度降低(BMD)风险增加之间的关联的证据并不一致。我们的目的是对 AB 与骨折和骨质疏松症或 BMD 降低相关的观察性研究进行系统评价,并对纳入的研究进行方法学评估。
我们检索了 MEDLINE、EMBASE、科学引文索引和 CENTRAL 以及数据库成立以来的灰色文献,直到 2020 年 8 月。纳入标准为:观察性设计,通过量表测量 AB 暴露,任何类型的骨折或骨质疏松症或 BMD 降低作为结局,以及报告暴露与结局之间关联的测量方法。未对时间、语言或数据类型施加任何限制。两名评审员独立进行了合格性和偏倚风险评估以及数据提取。使用纽卡斯尔-渥太华量表和 RTI 项目库评估纳入研究的偏倚风险。
纳入的 9 项研究中,大多数研究的偏倚风险较低,但方法学存在异质性。没有研究使用新用户设计。有 7 项研究报告 AB 与骨折风险增加有关。在使用抗胆碱能风险量表(ARS)的 4 项研究中,ARS=1 时骨折风险增加 2-61%,ARS=2 时增加 0-97%,ARS=3 时增加 19-84%,ARS≥4 时增加 56-96%;在 3 项研究中,ARS 被汇总,ARS=1-2 时风险增加 39%,ARS=2-3 时风险增加 17%。有 2 项研究报告最高 AB 类别的骨折风险增加 14%和 52%,有 1 项研究报告住院期间 ARS 增加≥3 与骨折风险增加 321%有关。有 2 项研究未发现 AB 与骨折之间存在关联。仅在 2 项研究中可以评估 AB 与骨质疏松症或 BMD 降低之间的关联,一项研究报告 Ward 三角区的 BMD 降低风险增加,另一项研究报告 AB 和股骨颈的 BMD T 评分变化之间无关联。
我们的研究表明 AB 与骨折风险增加之间存在关联,并且在使用 ARS 的研究中可能存在剂量-暴露梯度。由于研究数量少且方法学异质性,需要进行更多的研究。我们进行了一项研究,调查与抗胆碱能负担相关的骨折风险,这是服用一种或多种具有抗胆碱能活性的药物的结果。我们的研究结果表明,经历抗胆碱能负担的人可能有更高的骨折风险。但是,由于我们只能纳入 9 项研究,因此需要进行更多类似方法的研究。