Stewart Carrie, Taylor-Rowan Martin, Soiza Roy L, Quinn Terence J, Loke Yoon K, Myint Phyo Kyaw
Ageing Clinical and Experimental Research (ACER) Group, Institute of Applied Health Sciences, University of Aberdeen, Rm 1.128, Polwarth Building, Foresterhill Health Campus, Aberdeen, AB25 2ZD, UK.
Institute of Cardiovascular and Medical Sciences, University of Glasgow, Glasgow, UK.
Ther Adv Drug Saf. 2021 May 31;12:20420986211016645. doi: 10.1177/20420986211016645. eCollection 2021.
Several adverse outcomes have been associated with anticholinergic burden (ACB), and these risks increase with age. Several approaches to measuring this burden are available but, to date, no comparison of their prognostic abilities has been conducted. This PROSPERO-registered systematic review (CRD42019115918) compared the evidence behind ACB measures in relation to their ability to predict risk of falling in older people.
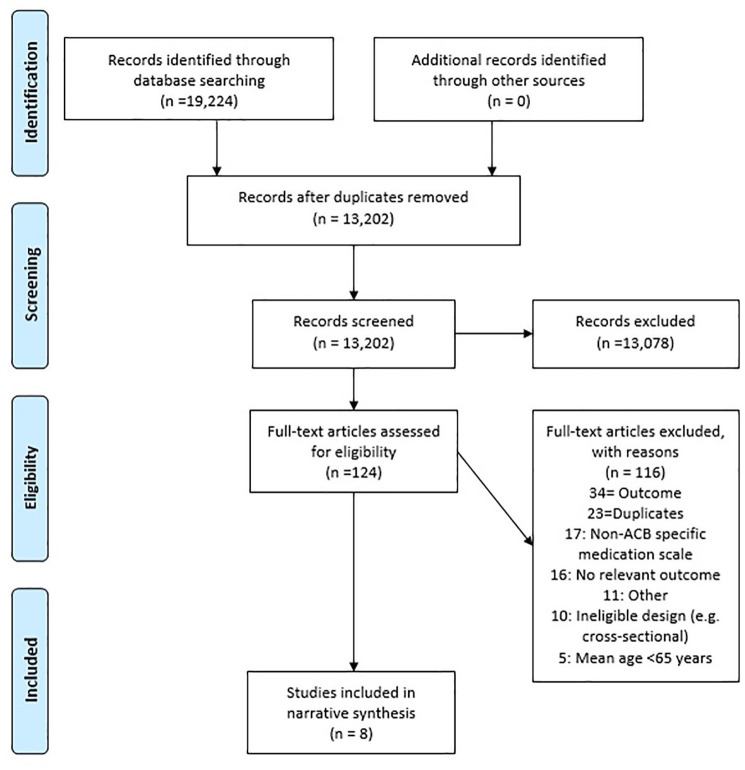
Medline (OVID), EMBASE (OVID), CINAHL (EMBSCO) and PsycINFO (OVID) were searched using comprehensive search terms and a validated search filter for prognostic studies. Inclusion criteria included: participants aged 65 years and older, use of one or more ACB measure(s) as a prognostic factor, cohort or case-control in design, and reporting falls as an outcome. Risk of bias was assessed using the Quality in Prognosis Studies (QUIPS) tool.
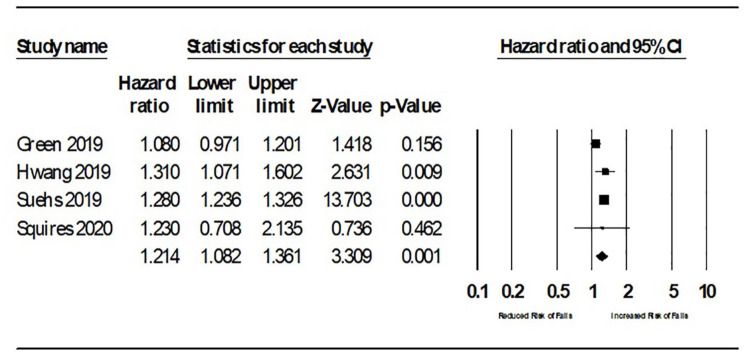
Eight studies reporting temporal associations between ACB and falls were included. All studies were rated high risk of bias in ⩾1 QUIPS tool categories, with five rated high risk ⩾3 categories. All studies (274,647 participants) showed some degree of association between anticholinergic score and increased risk of falls. Findings were most significant with moderate to high levels of ACB. Most studies (6/8) utilised the anticholinergic cognitive burden scale. No studies directly compared two or more ACB measures and there was variation in how falls were measured for analysis.
The evidence supports an association between moderate to high ACB and risk of falling in older people, but no conclusion can be made regarding which ACB scale offers best prognostic value in older people.
One third of older people will experience a fall. Falls have many consequences including fractures, a loss of independence and being unable to enjoy life. Many things can increase the chances of having a fall. This includes some medications. One type of medication, known as anticholinergic medication, may increase the risk of falls. These medications are used to treat common health issues including depression and bladder problems. Anticholinergic burden is the term used to describe the total effects from taking these medications. Some people may use more than one of these medications. This would increase their anticholinergic burden. It is possible that reducing the use of these medications could reduce the risk of falls. We need to carry out studies to see if this is possible. To do this, we need to be able to measure anticholinergic burden. There are several scales available, but we do not know which is best. We wanted to answer: 'Which anticholinergic scale is best at predicting the risk of falling in older people?'. We reviewed studies that could answer this. We did this in a systematic way to capture all published studies. We restricted the search in several ways. We only included studies relevant to our question. We found eight studies. We learned that people who are moderate to high users of these medications (often people who will use more than one of these medications) had a higher risk of falling. It was less clear if people who have a lower burden (often people who only use one of these medications) had an increased risk of falling. The low number of studies prevented us from determining if one scale was better than another. These findings suggest that we should reduce use of these medications. This could reduce the number falls and improve the well-being of older people.
抗胆碱能负担(ACB)与多种不良后果相关,且这些风险会随着年龄增长而增加。目前有多种测量这种负担的方法,但迄今为止,尚未对它们的预测能力进行比较。这项在PROSPERO注册的系统评价(CRD42019115918)比较了ACB测量方法在预测老年人跌倒风险方面的证据。
使用全面的检索词和经过验证的预后研究检索过滤器,对Medline(OVID)、EMBASE(OVID)、CINAHL(EMBSCO)和PsycINFO(OVID)进行检索。纳入标准包括:年龄在65岁及以上的参与者、使用一种或多种ACB测量方法作为预后因素、设计为队列研究或病例对照研究、并将跌倒作为结局进行报告。使用预后研究质量(QUIPS)工具评估偏倚风险。
纳入了八项报告ACB与跌倒之间时间关联的研究。所有研究在至少1个QUIPS工具类别中被评为高偏倚风险,其中五项在至少3个类别中被评为高偏倚风险。所有研究(274,647名参与者)均显示抗胆碱能评分与跌倒风险增加之间存在一定程度的关联。在中度至高度ACB水平下,研究结果最为显著。大多数研究(6/8)使用了抗胆碱能认知负担量表。没有研究直接比较两种或更多种ACB测量方法,并且在分析跌倒的测量方式上存在差异。
证据支持中度至高度ACB与老年人跌倒风险之间存在关联,但对于哪种ACB量表在老年人中具有最佳预后价值尚无定论。
三分之一的老年人会经历跌倒。跌倒会带来许多后果,包括骨折、失去独立性以及无法享受生活。许多因素会增加跌倒的几率。这包括一些药物。一种称为抗胆碱能药物的药物类型可能会增加跌倒风险。这些药物用于治疗常见的健康问题,包括抑郁症和膀胱问题。抗胆碱能负担是用于描述服用这些药物的总体影响的术语。有些人可能会使用不止一种这类药物。这会增加他们的抗胆碱能负担。减少这些药物的使用有可能降低跌倒风险。我们需要开展研究以确定这是否可行。为此,我们需要能够测量抗胆碱能负担。有几种量表可供使用,但我们不知道哪种最好。我们想回答:“哪种抗胆碱能量表最能预测老年人的跌倒风险?”。我们对能够回答这个问题的研究进行了综述。我们以系统的方式进行,以获取所有已发表的研究。我们通过多种方式限制了检索。我们只纳入与我们问题相关的研究。我们找到了八项研究。我们了解到,这些药物的中度至高度使用者(通常是使用不止一种这类药物 的人)跌倒风险更高。负担较低的人(通常是仅使用一种这类药物的人)跌倒风险是否增加则不太明确。研究数量较少使我们无法确定一种量表是否优于另一种。这些发现表明我们应该减少这些药物的使用。这可以减少跌倒次数并改善老年人的健康状况。