School of Medicine, Klinikum rechts der Isar, Department of Nephrology, Technical University of Munich, Ismaninger Str. 22, 81675, Munich, Germany.
School of Medicine, Klinikum rechts der Isar, Division of Rheumatology, Ismaninger Straße 22, 81675, Munich, Germany.
Sci Rep. 2020 Oct 26;10(1):18277. doi: 10.1038/s41598-020-75260-w.
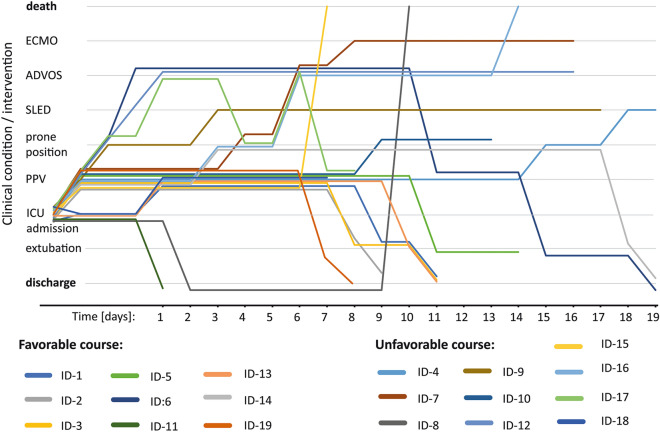
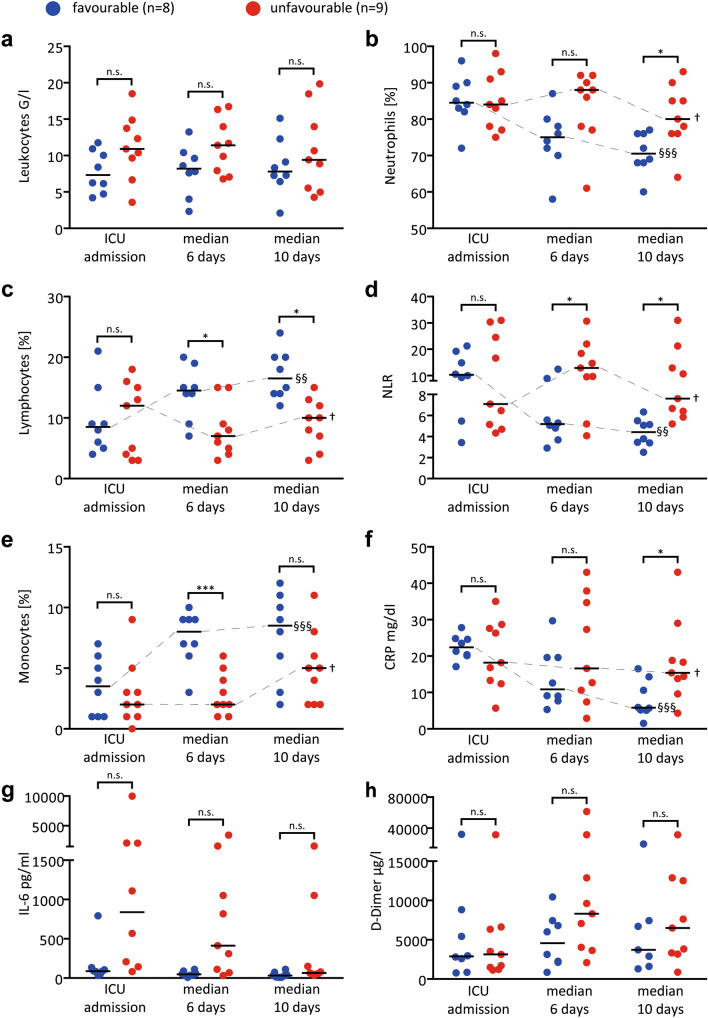
Severe COVID-19 associated respiratory failure, poses the one challenge of our days. Assessment and treatment of COVID-19 associated hyperinflammation may be key to improve outcomes. It was speculated that in subgroups of patients secondary hemophagocytic lymphohistiocytosis (sHLH) or cytokine release syndrome (CRS) with features of macrophage activation syndrome might drive severe disease trajectories. If confirmed, profound immunosuppressive therapy would be a rationale treatment approach. Over a median observation period of 11 (IQR: 8; 16) days, 19 consecutive confirmed severe COVID-19-patients admitted to our intensive-care-unit were tested for presence of sHLH by two independent experts. HScores and 2004-HLH diagnostic criteria were assessed. Patients were grouped according to short-term clinical courses: discharge from ICU versus ongoing ARDS or death at time of analysis. The median HScore at admission was 157 (IQR: 98;180), without the key clinical triad of HLH, i.e. progressive cytopenia, persistent fever and organomegaly. Independent expert chart review revealed the absence of sHLH in all cases. No patient reached more than 3/6 of modified HLH 2004 criteria. Nevertheless, patients presented hyperinflammation with peripheral neutrophilic signatures (neutrophil/lymphocyte-ratio > 3.5). The latter best paralleled their short-term clinical courses, with declining relative neutrophil numbers prior to extubation (4.4, [IQR: 2.5;6.3]; n = 8) versus those with unfavourable courses (7.6, [IQR: 5.2;31], n = 9). Our study rules out virus induced sHLH as the leading cause of most severe-COVID-19 trajectories. Instead, an associated innate neutrophilic hyperinflammatory response or virus-associated-CRS appears dominant in patients with an unfavourable clinical course. Therapeutic implications are discussed.
严重的 COVID-19 相关呼吸衰竭是我们目前面临的挑战之一。评估和治疗 COVID-19 相关的过度炎症可能是改善预后的关键。有人推测,在具有巨噬细胞活化综合征特征的继发性噬血细胞性淋巴组织细胞增生症(sHLH)或细胞因子释放综合征(CRS)亚组患者中,可能会导致严重的疾病轨迹。如果得到证实,深度免疫抑制治疗将是一种合理的治疗方法。在 19 名连续确诊的 COVID-19 重症患者中,中位观察期为 11 天(IQR:8;16),两名独立专家通过两种方法对 sHLH 的存在进行了测试。评估了 HScores 和 2004-HLH 诊断标准。根据短期临床病程将患者分为两组:从 ICU 出院与持续 ARDS 或分析时死亡。入院时的中位数 HScore 为 157(IQR:98;180),没有 HLH 的关键临床三联征,即进行性血细胞减少、持续发热和器官肿大。独立专家的图表审查显示所有病例均不存在 sHLH。没有患者达到 2004 年改良 HLH 标准的 3/6 以上。然而,所有患者均表现出炎症反应,外周中性粒细胞特征明显(中性粒细胞/淋巴细胞比值>3.5)。后者与他们的短期临床病程最为相似,在拔管前中性粒细胞数量下降(4.4,IQR:2.5;6.3;n=8),而那些病情不佳的患者(7.6,IQR:5.2;31,n=9)。我们的研究排除了病毒引起的 sHLH 作为大多数严重 COVID-19 轨迹的主要原因。相反,在病情不佳的患者中,与先天中性粒细胞过度炎症反应或病毒相关的 CRS 相关的噬血细胞性淋巴组织细胞增生症似乎更为常见。讨论了治疗意义。