State Key Laboratory of Cardiovascular Disease, Fu Wai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences, Peking Union Medical College, BeiLiShi Road 167, Beijing, 100037, China.
Division of Cardiology, The Fifth Hospital of Wuhan & Cardiovascular Insititute of Jianghan University, Wuhan, 430050, China.
BMC Cardiovasc Disord. 2020 Oct 28;20(1):465. doi: 10.1186/s12872-020-01743-3.
Total leukocyte and differential Leukocyte counts are prognostic indictors in patients with coronary artery disease (CAD). However, there is no data available regarding their prognostic utility in very old patients with acute myocardial infarction (AMI). The aim of this study is to investigate the potential role of different leukocyte parameters in predicting the mortality among very old patients with AMI.
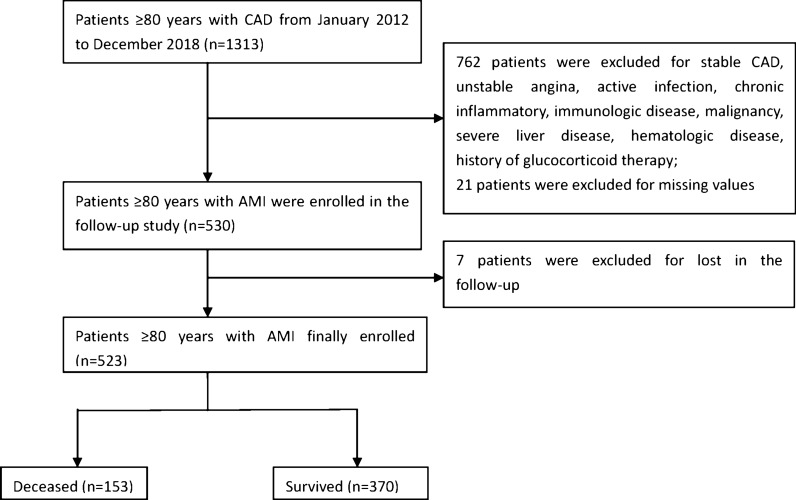
A total of 523 patients aged over 80 years with AMI were consecutively enrolled into this study. Leukocyte and its subtypes were obtained at admission in each patient. The primary study endpoint was cardiovascular mortality. Patients were followed up for an average of 2.2 years and 153 patients died. The associations of leukocyte parameters with mortality were assessed using Cox regression analyses. The concordance index was calculated to test the model efficiency.
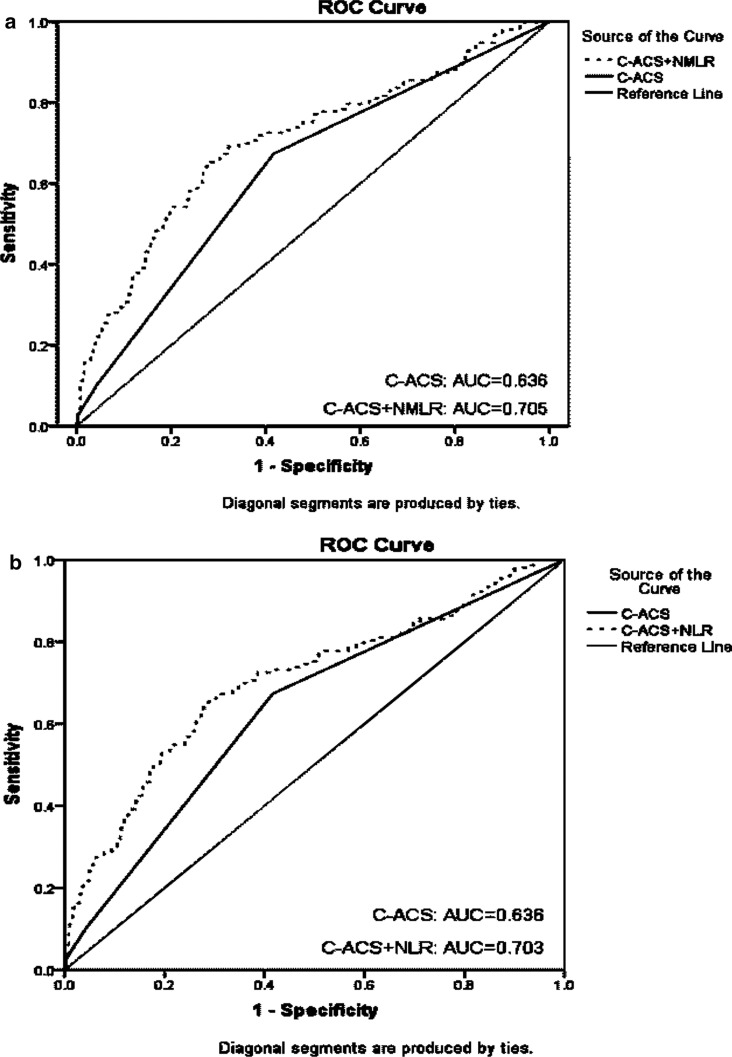
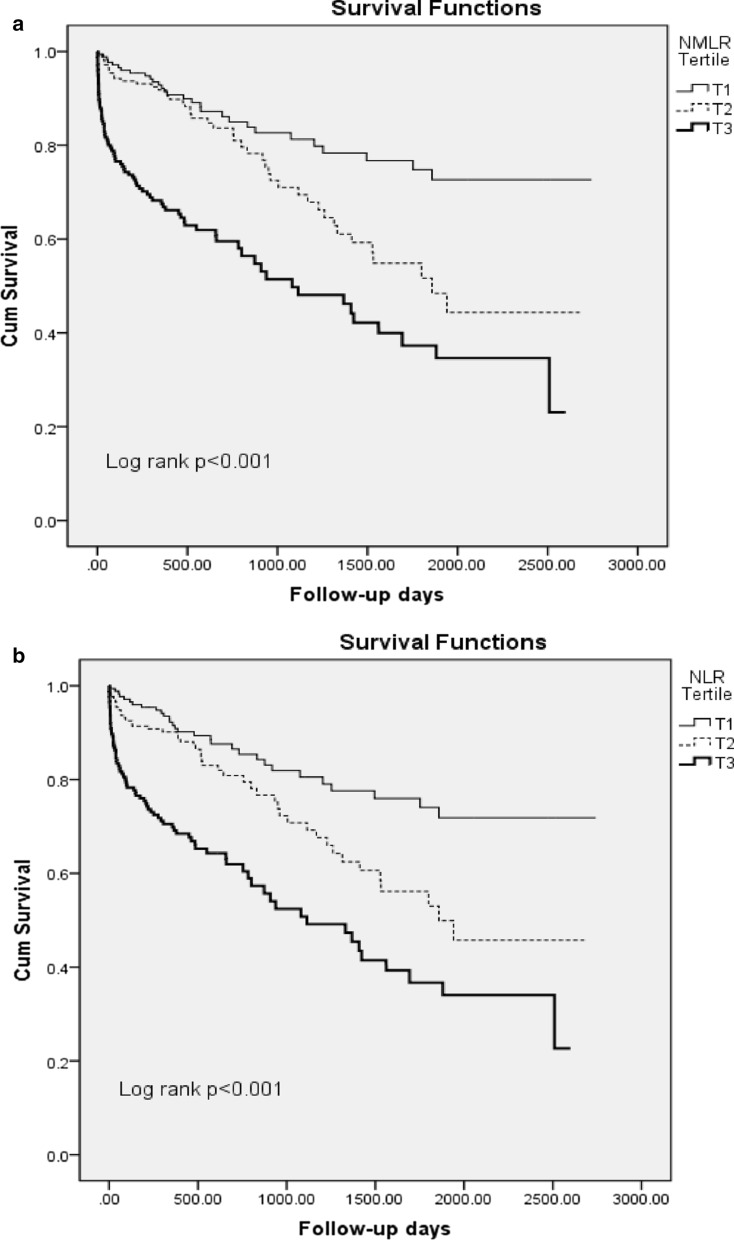
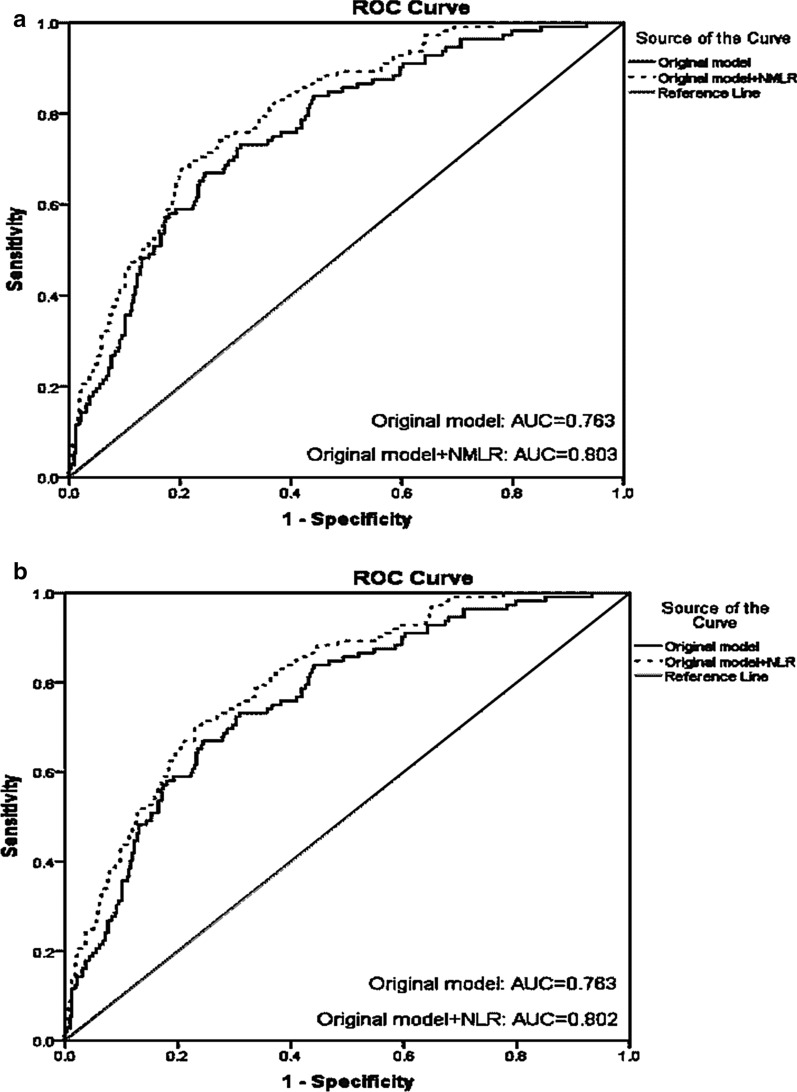
In multivariable regression analysis, neutrophils-plus-monocytes-to-lymphocytes ratio (NMLR) and neutrophils-to-lymphocytes ratio (NLR) were two most significant predictors of mortality among all the leukocyte parameters (HR = 3.21, 95% CI 1.75-5.35; HR = 2.79, 95% CI 1.59-4.88, respectively, all p < 0.001, adjusted for age, male gender, body mass index, family history of CAD, smoking, hypertension, diabetes mellitus, high-density lipoprotein cholesterol (HDL-C), non-HDL-C, high sensitivity C-reactive protein, creatinine, left ventricular ejection fraction, troponin I, use of statin, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, and percutaneous coronary intervention). Furthermore, adding NMLR and NLR into the Cox model increased the C-statistic by 0.038 and 0.037 respectively, which were more significant than that of other leukocyte parameters. Besides, addition of NMLR and NLR to the Canada Acute Coronary Syndrome Risk Score model also increased the C-statistic by 0.079 and 0.077 respectively.
Our data firstly indicated that most leukocyte subtypes were independent markers for the mortality in very old patients with AMI, while NMLR and NLR appeared to be more effective.
白细胞总数和白细胞分类计数是冠心病患者的预后指标。然而,关于其在急性心肌梗死(AMI)高龄患者中的预后价值尚无数据。本研究旨在探讨不同白细胞参数在预测高龄 AMI 患者死亡率中的潜在作用。
本研究共连续纳入 523 名年龄在 80 岁以上的 AMI 患者。每位患者入院时均检测白细胞及其亚群。主要研究终点为心血管死亡率。患者平均随访 2.2 年,共有 153 人死亡。使用 Cox 回归分析评估白细胞参数与死亡率的相关性。计算一致性指数以检验模型效率。
多变量回归分析显示,中性粒细胞加单核细胞与淋巴细胞比值(NMLR)和中性粒细胞与淋巴细胞比值(NLR)是所有白细胞参数中与死亡率最显著相关的两个指标(HR=3.21,95%CI 1.75-5.35;HR=2.79,95%CI 1.59-4.88,均 P<0.001,调整年龄、男性、体重指数、CAD 家族史、吸烟、高血压、糖尿病、高密度脂蛋白胆固醇(HDL-C)、非高密度脂蛋白胆固醇(non-HDL-C)、高敏 C 反应蛋白、肌酐、左心室射血分数、肌钙蛋白 I、他汀类药物、血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂和经皮冠状动脉介入治疗)。此外,将 NMLR 和 NLR 纳入 Cox 模型可使 C 统计量分别增加 0.038 和 0.037,比其他白细胞参数更显著。此外,将 NMLR 和 NLR 添加到加拿大急性冠状动脉综合征风险评分模型中也分别使 C 统计量增加 0.079 和 0.077。
本研究数据首次表明,大多数白细胞亚型是高龄 AMI 患者死亡率的独立标志物,而 NMLR 和 NLR 似乎更为有效。