Department of Internal Medicine and Medical Specialties (DiMI), School of Medicine, University of Genova, Genova, Liguria, Italy; Department of Medical Oncology, U.O.C Clinica di Oncologia Medica, IRCCS Ospedale Policlinico San Martino, Genova, Italy.
Physiopatology of Human Reproduction Unit, IRCCS Ospedale Policlinico San Martino, Genova, Italy.
ESMO Open. 2020 Oct;5(Suppl 4):e000771. doi: 10.1136/esmoopen-2020-000771.
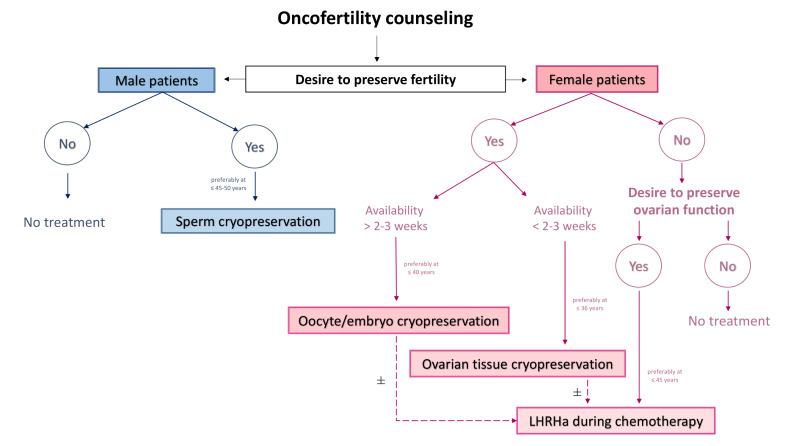
Survivorship is an area of paramount importance to be addressed as early as possible after cancer diagnosis by all health care providers. On this regard, cancer care in young patients often poses several age-related considerations among which fertility and pregnancy-related issues have a crucial role. According to the available guidelines on the topic, all patients with cancer diagnosed during their reproductive years should be provided a proper oncofertility counselling before starting anticancer treatments. This is an important step in order to inform patients about the potential treatment-induced gonadotoxicity and the available strategies for fertility preservation so that they can be referred as early as possible to fertility specialists if potentially interested in these options.In this manuscript, we aim to provide an up to date overview on the available efficacy and safety data with the main strategies for fertility preservation in male and female cancer patients in order to help optimising the oncofertility counselling performed by healthcare providers involved in cancer care and dealing with young patients. In male patients with cancer, sperm cryopreservation is the standard technique for fertility preservation. Oocyte/embryo cryopreservation, ovarian tissue cryopreservation and temporary ovarian suppression with luteinising hormone-releasing hormone agonists during chemotherapy are the main options in female patients with cancer.A multidisciplinary management building a strong network between fertility and oncology/haematology units is crucial to properly address fertility care in all young patients with cancer, at both diagnosis and during oncologic follow-up. Discussing fertility and pregnancy-related issues with young patients with cancer has to be considered mandatory nowadays keeping in mind that returning to a normal life (including the possibility to have a family and to live with as few side effects as possible) should be considered an important ambition in cancer care in the 21st century .
生存问题是癌症诊断后所有医疗保健提供者都应尽早关注的一个至关重要的领域。在这方面,年轻患者的癌症治疗常常涉及到几个与年龄相关的考虑因素,其中与生育和妊娠相关的问题起着至关重要的作用。根据该主题的现有指南,所有在生育年龄期间被诊断患有癌症的患者在开始抗癌治疗之前都应接受适当的肿瘤生育咨询。这是一个重要的步骤,以便向患者告知潜在的治疗引起的性腺毒性以及可用的生育力保存策略,以便他们如果对这些选择感兴趣,可以尽早转介给生育专家。在本文中,我们旨在提供有关男性和女性癌症患者中可用的生育力保存主要策略的最新疗效和安全性数据的概述,以帮助优化参与癌症护理和治疗年轻患者的医疗保健提供者所进行的肿瘤生育咨询。对于患有癌症的男性患者,精子冷冻保存是生育力保存的标准技术。对于患有癌症的女性患者,卵母细胞/胚胎冷冻保存、卵巢组织冷冻保存以及在化疗期间使用促黄体生成素释放激素激动剂进行暂时卵巢抑制是主要选择。建立一个由生育和肿瘤/血液学单位组成的强大网络的多学科管理对于所有年轻癌症患者在诊断时和肿瘤随访期间的生育护理至关重要。与年轻的癌症患者讨论生育和妊娠相关问题,现在必须被视为强制性的,因为考虑到回到正常生活(包括有生育能力和尽可能少的副作用的可能性)应该被视为 21 世纪癌症治疗的一个重要目标。