Department of Public Health, Faculty of Health Sciences, Busitema University , Tororo, Uganda.
Centre for International Health, University of Bergen , Bergen, Norway.
Glob Health Action. 2020 Dec 31;13(1):1833510. doi: 10.1080/16549716.2020.1833510.
Breastfeeding is important for growth, development and survival of HIV exposed infants. Exclusive breastfeeding reduces the risk of morbidity, mortality and increases HIV free survival of infants. Evidence on risk factors for inappropriate breastfeeding in Northern Uganda is limited.
This study determined the risk factors for non-exclusivity of breastfeeding in the first 14 weeks of life.
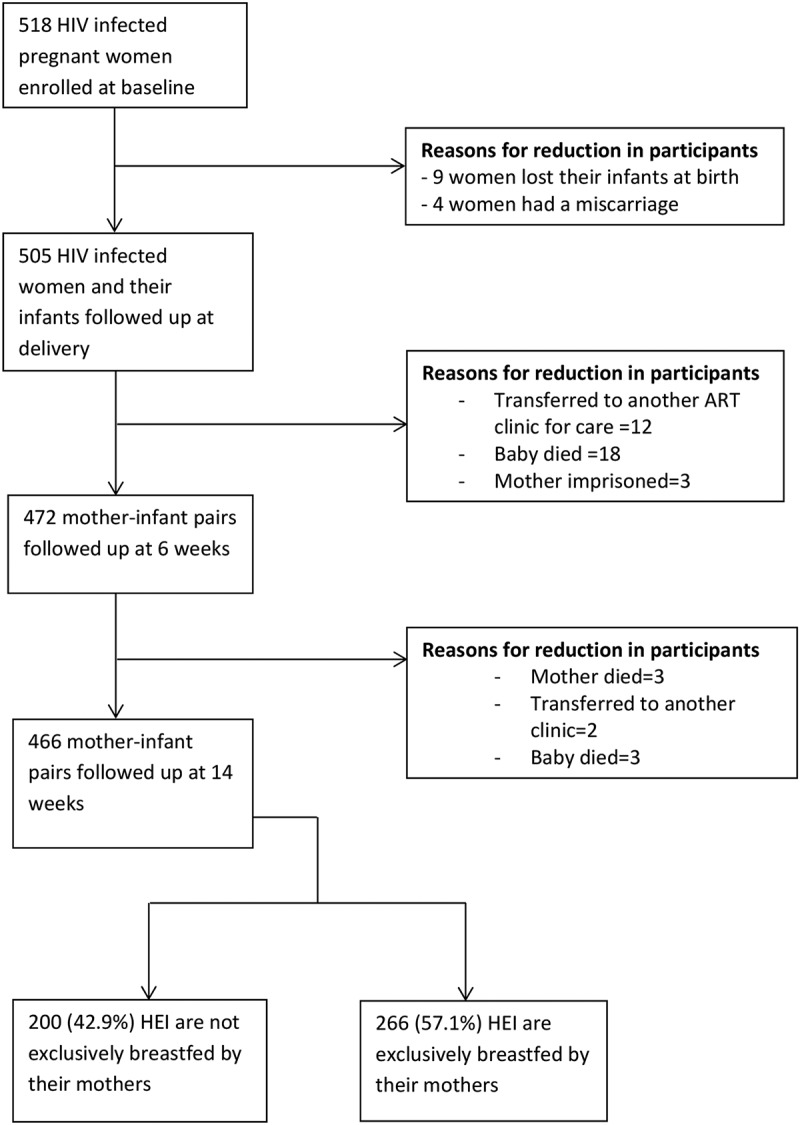
This prospective cohort study was conducted among 466 mother-infant pairs between August 2018 and February 2020 in Lira district, Northern Uganda. HIV infected pregnant women were enrolled and followed up at delivery, 6- and 14- weeks postpartum. We used a structured questionnaire to obtain data on socio-demographic, reproductive-related, HIV-related characteristics and exclusive breastfeeding. Data were analysed using Stata version 14.0 (StataCorp, College Station, Texas, USA.). We estimated adjusted risk ratios using modified Poisson regression models.
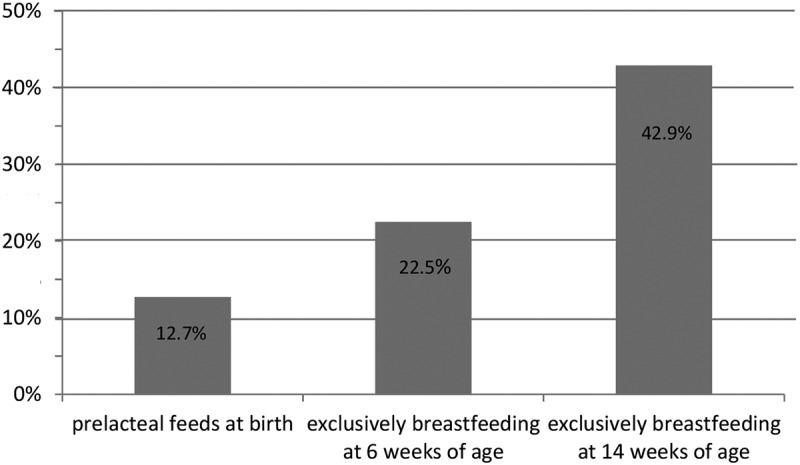
The proportion of HIV exposed infants that were exclusively breastfed reduced with increasing age. Risk factors for non-exclusive breastfeeding included infants being born to HIV infected women who: were in the highest socioeconomic strata (adjusted risk ratio = 1.5, 95%CI: 1.01- 2.1), whose delivery was supervised by a non-health worker (adjusted risk ratio = 1.6, 95%CI: 1.01- 2.7) and who had not adhered to their ART during pregnancy (adjusted risk ratio = 1.3, 95%CI: 1.01- 1.7).
HIV infected women: with highest socioeconomic status, whose delivery was not supervised by a health worker and who did not adhere to ART were less likely to practice exclusive breastfeeding. We recommend ART adherence and infant feeding counselling to be emphasised among HIV infected women who are at risk of having a home delivery, those with poor ART adherence and those of higher socioeconomic status. We also recommend integration of these services into other settings like homes, community and work places instead of limiting them to hospital settings.
HIV: Human Immunodeficiency Virus; ART: Antiretroviral therapy; HEI: HIV exposed infant; PMTCT: Prevention of mother-to-child transmission of HIV; MTCT: Mother-to-child transmission of HIV; AFASS: Acceptable, Feasible, Affordable, Sustainable and Safe; LRRH: Lira regional referral hospital; CI: confidence interval; ARR: Adjusted risk ratio; SD: Standard deviation; PCA: Principal component analysis.
母乳喂养对 HIV 暴露婴儿的生长、发育和生存至关重要。纯母乳喂养可降低发病率、死亡率,并提高婴儿的 HIV 存活率。关于北乌干达不适当母乳喂养风险因素的证据有限。
本研究旨在确定头 14 周内非纯母乳喂养的风险因素。
本前瞻性队列研究于 2018 年 8 月至 2020 年 2 月在北乌干达利拉区进行,共纳入 466 对母婴对。入组时 HIV 感染孕妇,并在分娩时、产后 6 周和 14 周进行随访。我们使用结构化问卷获取社会人口统计学、生殖相关、HIV 相关特征和纯母乳喂养数据。使用 Stata 版本 14.0(StataCorp,德克萨斯州学院站)分析数据。我们使用修正泊松回归模型估计调整后的风险比。
HIV 暴露婴儿的纯母乳喂养比例随年龄增加而降低。非纯母乳喂养的风险因素包括:HIV 感染产妇属于最高社会经济阶层(调整后的风险比为 1.5,95%CI:1.01-2.1)、分娩由非卫生工作者监督(调整后的风险比为 1.6,95%CI:1.01-2.7)和孕期未遵医嘱服用抗逆转录病毒药物(调整后的风险比为 1.3,95%CI:1.01-1.7)。
HIV 感染产妇:社会经济地位较高、分娩未由卫生工作者监督、未遵医嘱服用抗逆转录病毒药物的产妇,更不可能进行纯母乳喂养。我们建议对有在家分娩风险、抗逆转录病毒药物依从性差和社会经济地位较高的 HIV 感染产妇,加强抗逆转录病毒药物依从性和婴儿喂养咨询。我们还建议将这些服务整合到家庭、社区和工作场所等其他环境中,而不是将其仅限于医院环境。
HIV:人类免疫缺陷病毒;ART:抗逆转录病毒治疗;HEI:HIV 暴露婴儿;PMTCT:预防母婴传播 HIV;MTCT:母婴传播 HIV;AFASS:可接受、可行、负担得起、可持续和安全;LRRH:利拉地区转诊医院;CI:置信区间;ARR:调整后的风险比;SD:标准差;PCA:主成分分析。