Hong Jin, Wu Jiayi, Huang Ou, He Jianrong, Zhu Li, Chen Weiguo, Li Yafen, Chen Xiaosong, Shen Kunwei
Department of General Surgery, Comprehensive Breast Health Center, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200025, PR China.
J Cancer. 2020 Oct 6;11(23):6916-6924. doi: 10.7150/jca.46805. eCollection 2020.
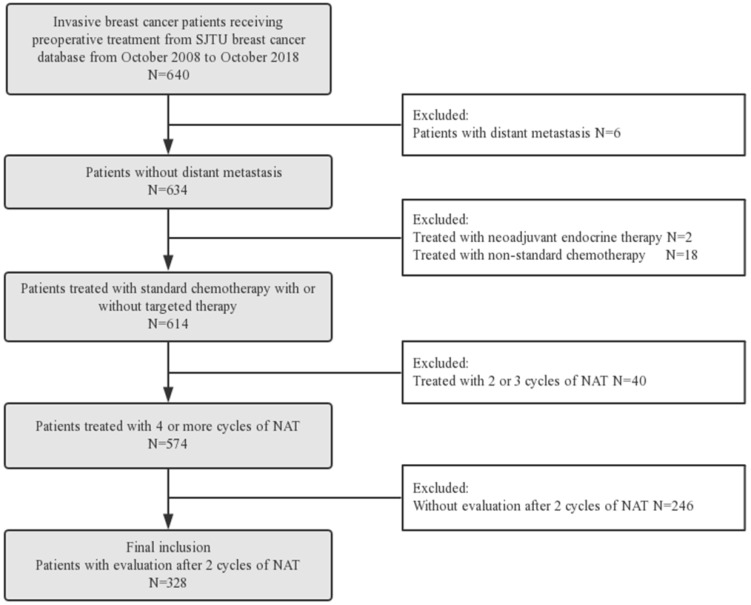
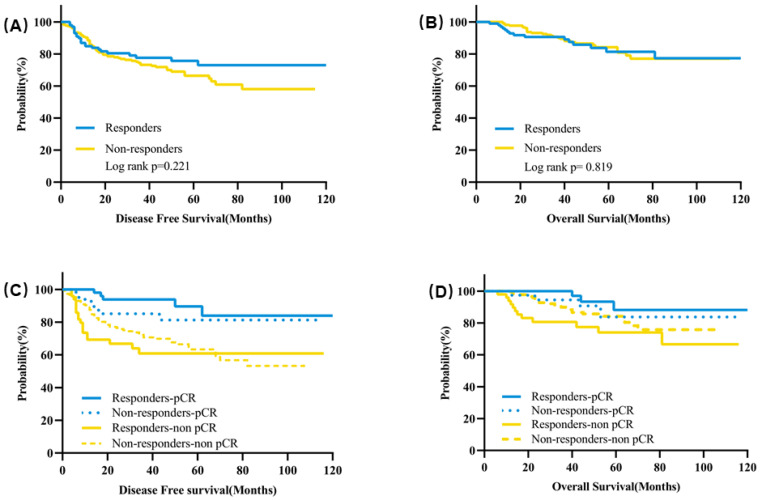
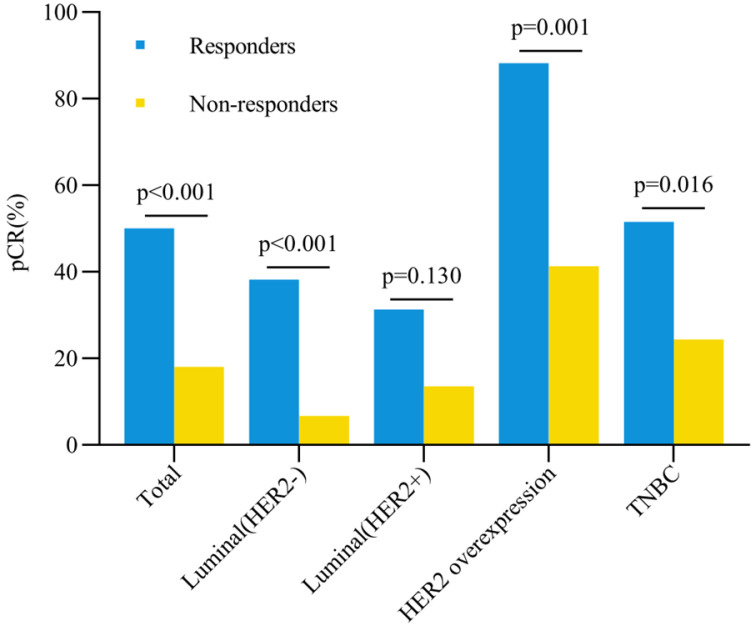
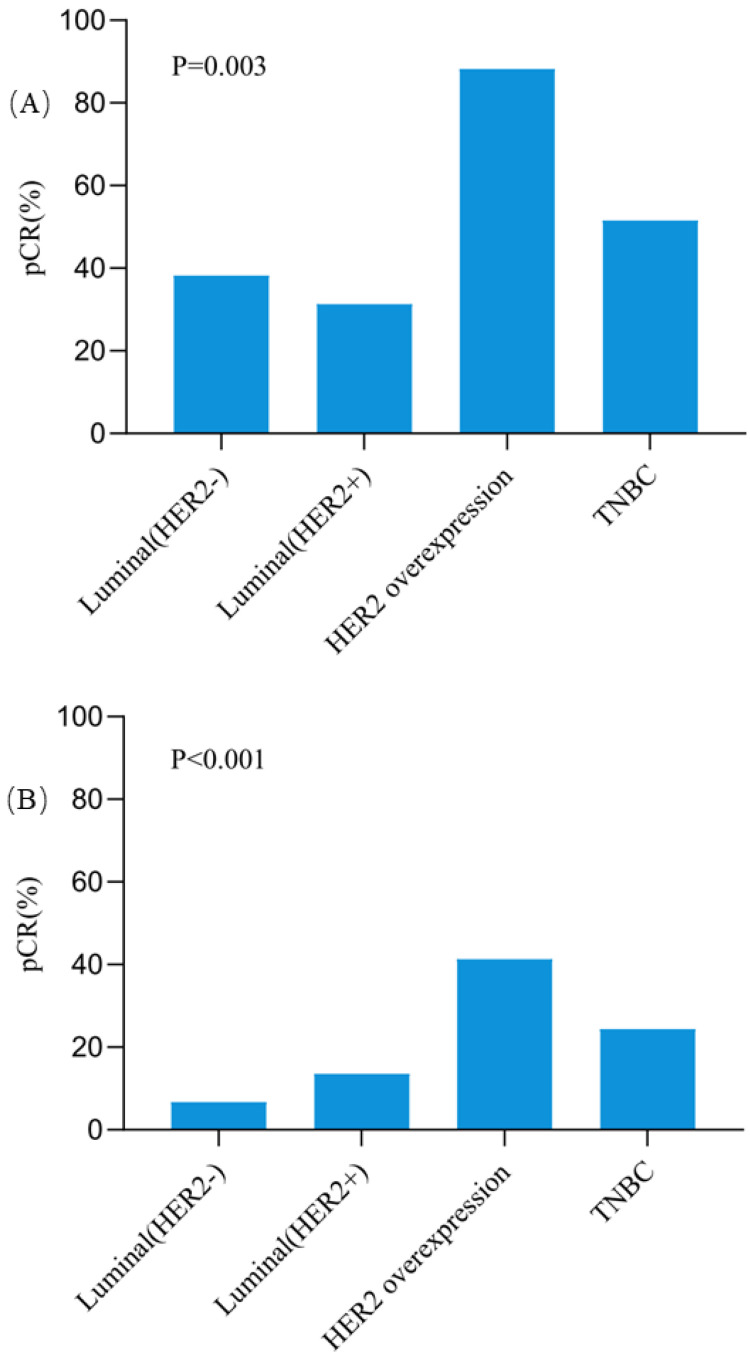
To evaluate the association of clinical early response and pathological complete remission (pCR) in breast cancer patients with different molecular subtypes. Breast cancer patients who received neoadjuvant treatment (NAT) with clinical early response assessment from October 2008 to October 2018 were retrospectively analyzed. Clinical early response was defined as tumor size decreasing ≥30% evaluated by ultrasound after two cycles of NAT. Chi-square test was used to compare the pCR rates between the responder and non-responder groups with different molecular subtypes. Multivariate logistic regression was used to identify independent factors associated with the pCR. A total of 328 patients were included: 100 responders and 228 non-responders. The progesterone receptor (PR) expression was an independent factor associated with clinical early response (OR=2.39, 95%CI=1.41-4.05, =0.001). The pCR rate of breast was 50.0% for responders and 18.0% for non-responders (<0.001). Regarding different molecular subtypes, responders had higher pCR rates than non-responders for patients with HER2 overexpression (OR=10.66, 95%CI=2.18-52.15, =0.001), triple negative (OR=3.29, 95%CI=1.23-8.84, =0.016) and Luminal (HER2-) subtypes (OR=8.58, 95%CI=3.05-24.10, <0.001) respectively. Moreover, pCR rate can be achieved as high as 88.2% in HER2 overexpression patients with early clinical response, which was significantly higher than patients without early response (41.3%, =0.001). Multivariate analysis showed that clinical early response was an independent factor associated with the pCR rate (OR=4.87, 95%CI=2.72-8.72, <0.001). Early response was significantly associated with a higher pCR rate in breast cancer patients receiving NAT, especially for patients with HER2 overexpression subtype, which warrants further clinical evaluation.
评估不同分子亚型乳腺癌患者临床早期反应与病理完全缓解(pCR)之间的关联。回顾性分析2008年10月至2018年10月期间接受新辅助治疗(NAT)并进行临床早期反应评估的乳腺癌患者。临床早期反应定义为在两个周期的NAT后通过超声评估肿瘤大小减小≥30%。采用卡方检验比较不同分子亚型的反应者和无反应者组之间的pCR率。使用多因素逻辑回归来确定与pCR相关的独立因素。共纳入328例患者:100例反应者和228例无反应者。孕激素受体(PR)表达是与临床早期反应相关的独立因素(OR=2.39,95%CI=1.41-4.05,P=0.001)。反应者的乳腺癌pCR率为50.0%,无反应者为18.0%(P<0.001)。对于不同分子亚型,HER2过表达患者(OR=10.66,95%CI=2.18-52.15,P=0.001)、三阴性患者(OR=3.29,95%CI=1.23-8.84,P=0.016)和Luminal(HER2-)亚型患者(OR=8.58,95%CI=3.05-24.10,P<0.001)中,反应者的pCR率均高于无反应者。此外,HER2过表达且有早期临床反应的患者pCR率可高达88.2%,显著高于无早期反应的患者(41.3%,P=0.001)。多因素分析显示临床早期反应是与pCR率相关的独立因素(OR=4.87,95%CI=2.72-8.72,P<0.001)。早期反应与接受NAT的乳腺癌患者较高的pCR率显著相关,尤其是HER2过表达亚型患者,这值得进一步的临床评估。