Chen Tao, Bai Linfu, Hu Wenhui, Han Xiaoli, Duan Jun
The Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China.
Can Respir J. 2020 Oct 13;2020:8885464. doi: 10.1155/2020/8885464. eCollection 2020.
Risk factors for noninvasive ventilation (NIV) failure after initial success are not fully clear in patients with acute exacerbation of chronic obstructive pulmonary disease (COPD).
Patients who received NIV beyond 48 h due to acute exacerbation of COPD were enrolled. However, we excluded those whose pH was higher than 7.35 or PaCO was less than 45 mmHg which was measured before NIV. Late failure of NIV was defined as patients required intubation or died during NIV after initial success.
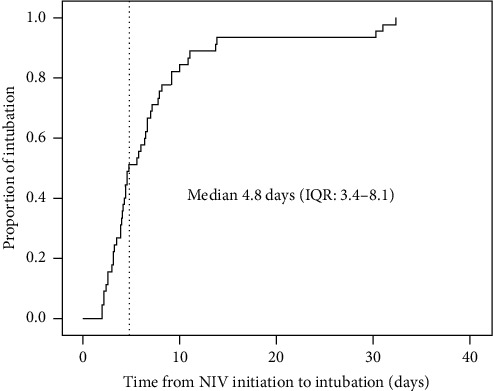
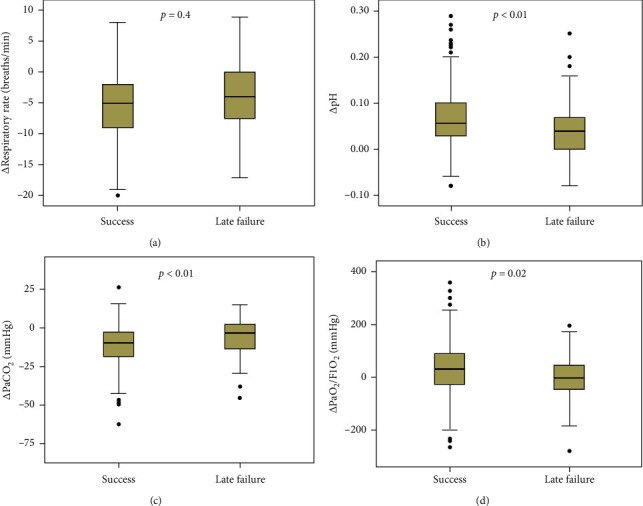
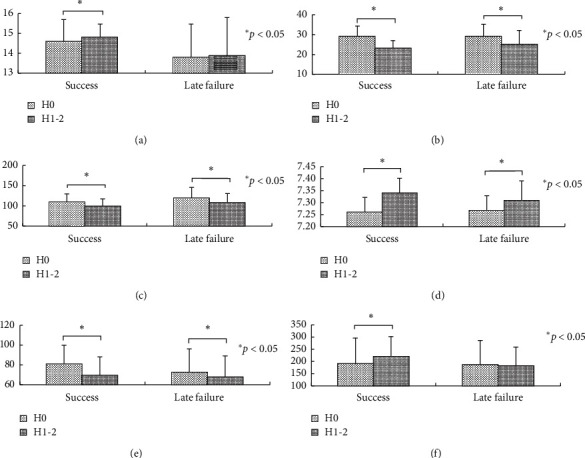
We enrolled 291 patients in this study. Of them, 48 (16%) patients experienced late NIV failure (45 received intubation and 3 died during NIV). The median time from initiation of NIV to intubation was 4.8 days (IQR: 3.4-8.1). Compared with the data collected at initiation of NIV, the heart rate, respiratory rate, pH, and PaCO significantly improved after 1-2 h of NIV both in the NIV success and late failure of NIV groups. Nosocomial pneumonia (odds ratio (OR) = 75, 95% confidence interval (CI): 11-537), heart rate at initiation of NIV (1.04, 1.01-1.06 beat per min), and pH at 1-2 h of NIV (2.06, 1.41-3.00 per decrease of 0.05 from 7.35) were independent risk factors for late failure of NIV. In addition, the Glasgow coma scale (OR = 0.50, 95% CI: 0.34-0.73 per one unit increase) and PaO/FiO (0.992, 0.986-0.998 per one unit increase) were independent protective factors for late failure of NIV. In addition, patients with late failure of NIV had longer ICU stay (median 9.5 vs. 6.6 days) and higher hospital mortality (92% vs. 3%) compared with those with NIV success.
Nosocomial pneumonia; heart rate at initiation of NIV; and consciousness, acidosis, and oxygenation at 1-2 h of NIV were associated with late failure of NIV in patients with COPD exacerbation. And, late failure of NIV was associated with increased hospital mortality.
在慢性阻塞性肺疾病(COPD)急性加重患者中,无创通气(NIV)初始成功后失败的危险因素尚不完全清楚。
纳入因COPD急性加重接受NIV超过48小时的患者。然而,我们排除了那些NIV前测量的pH值高于7.35或动脉血二氧化碳分压(PaCO)低于45 mmHg的患者。NIV晚期失败定义为患者在NIV初始成功后需要插管或在NIV期间死亡。
本研究共纳入291例患者。其中,48例(16%)患者发生NIV晚期失败(45例接受插管,3例在NIV期间死亡)。从开始NIV到插管的中位时间为4.8天(四分位间距:3.4 - 8.1天)。与NIV开始时收集的数据相比,NIV成功组和NIV晚期失败组在NIV 1 - 2小时后心率、呼吸频率、pH值和PaCO均有显著改善。医院获得性肺炎(比值比(OR)= 75,95%置信区间(CI):11 - 537)、NIV开始时的心率(1.04,1.01 - 1.06次/分钟)以及NIV 1 - 2小时时的pH值(2.06,pH值从7.35每降低0.05时为1.41 - 3.00)是NIV晚期失败的独立危险因素。此外,格拉斯哥昏迷量表(OR = 0.50,95% CI:每增加一个单位为0.34 - 0.73)和氧合指数(PaO₂/FiO₂,每增加一个单位为0.992,0.986 - 0.998)是NIV晚期失败的独立保护因素。此外,与NIV成功的患者相比,NIV晚期失败的患者入住重症监护病房(ICU)的时间更长(中位时间9.0天对6.6天)且医院死亡率更高(92%对3%)。
医院获得性肺炎、NIV开始时的心率以及NIV 1 - 2小时时的意识、酸中毒和氧合情况与COPD加重患者的NIV晚期失败相关。而且,NIV晚期失败与医院死亡率增加相关。